CASE 180
History: A 23-year-old woman presents with abdominal pain and diarrhea.
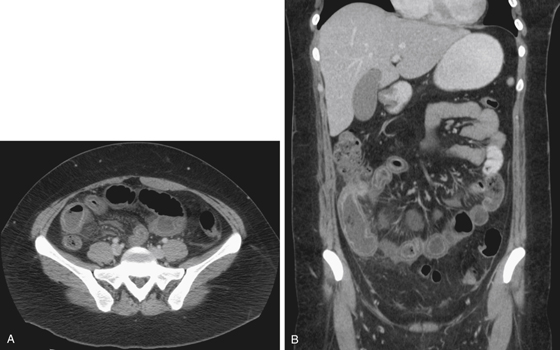
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. In this case, the thickened ileum has three layers with a middle low-attenuation layer. What is the name of this sign?
3. Which of the following statements regarding the CT halo sign is true?
A. The lucent layer is due to widening of the submucosa.
B. Intravenous contrast medium is required to render the lucent layer visible.
C. Halo sign of the colon is most likely due to Crohn’s disease.
D. Halo sign of the terminal ileum is diagnostic of Crohn’s disease.
4. Which of the following statements regarding patients with Crohn’s disease presenting after age 50 years is true?
A. Most elderly patients with Crohn’s disease are men.
B. About 10% to 15% of patients with Crohn’s disease present after age 50 years.
C. Crohn’s disease in elderly patients more frequently involves the small bowel.
D. Mortality is higher and response to treatment is poorer in elderly patients with Crohn’s disease.
ANSWERS
CASE 180
Intramural Fat in Crohn’s Disease
1. D and E
2. C
3. A
4. B
References
Ahualli J. The fat halo sign. Radiology. 2007;242(3):945-946.
Wills JS, Lobis IF, Denstman FJ. Crohn disease: state of the art. Radiology. 1997;202(3):597-610.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 294.
Comment
The ring of fat tissue seen in the submucosa of this patient is fast becoming an important CT sign of inflammatory bowel disease (see figures). Generally, the halo sign of submucosal fat is not specific for any particular disease, and it has been described in several inflammatory conditions, including Crohn’s disease and ulcerative colitis and some inflammatory processes including radiation enteritis. It also has been described in normal bowel. This is not the creeping fat sign described by pathologists and relating to the gross anatomy of Crohn’s disease, in which mesenteric fat around the diseased bowel becomes thickened and rubbery and appears to extend over the inflamed serosal surface similar to “fingers of fat” creeping across the surface of the bowel.
The halo sign (as seen in this case) is seen in gastrointestinal inflammatory conditions as a well-defined ring of submucosal lucency, usually of fat density. This sign has become more noticeable since the advent of high-resolution CT imaging. It has also been described in intestinal lymphangiectasia. Some authors think of the halo sign as nonspecific submucosal edema. It is difficult to measure Hounsfield numbers of the lucent ring.
Subsequent biopsy of this bowel showed this to be Crohn’s disease. Edema of the bowel wall usually affects all layers. The halo sign has been described in patients with no evidence of bowel disease. It may be a finding related to obesity in such cases. If one accepts the fact that the halo sign can represent either fat or a ring of edema, other possibilities must be considered, such as ischemic bowel or pseudomembranous colitis. Some authors have deemed the rings of lucency as a double halo sign when edema is seen between the mucosa and submucosa. Generally, a thin single fatty submucosal layer is another manifestation of bowel wall inflammation. In a young patient, such as in this case, with the halo sign involving the terminal ileum, Crohn’s disease must be considered first.






