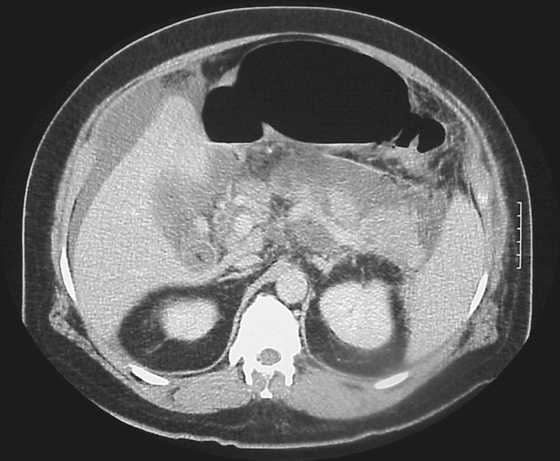
History: A 70-year-old man suffered severe epigastric pain 3 months ago. He now presents with 3 weeks of increasing vomiting and is unable to keep any solid food down.
1. Which of the following should be included in the differential diagnosis of the dominant imaging finding? (Choose all that apply.)
A. Superior mesenteric artery (SMA) syndrome
2. What is the most common primary malignant lesion of the duodenum?
3. Several viscera are related to the descending duodenum; therefore, a disease process in these viscera can involve the descending duodenum. Conversely, a disease process arising in the descending duodenum can spread to these viscera. Which of these viscera are not related to the descending duodenum?
4. What is the most common cause for duodenal inflammation?
A. Hyperacidity and peptic ulcer disease
ANSWERS
CASE 18
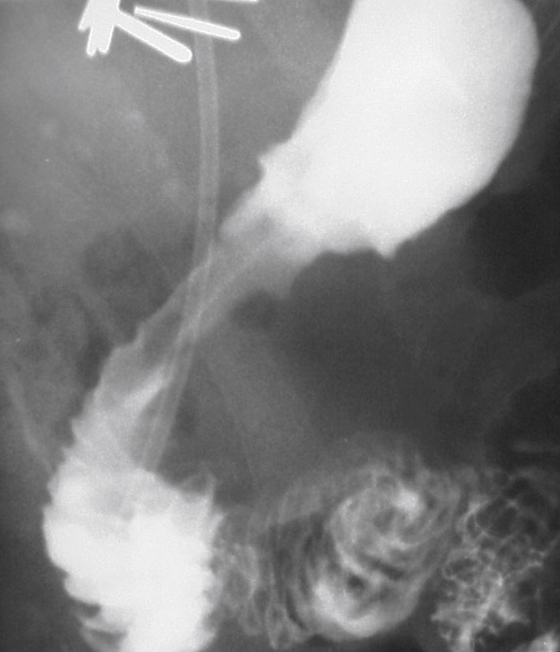
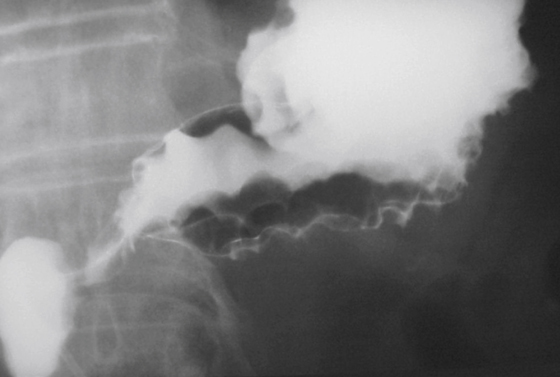
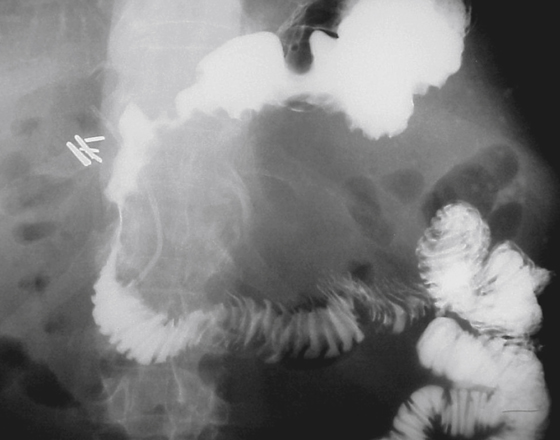
Duodenal Narrowing Secondary to Pancreatitis
1. B, C, D, and E
2. A
3. A
4. A
References
Bilimoria KY, Bentrem DJ, Wayne JD, et al: Small bowel cancer in the United States: changes in epidemiology, treatment, and survival over the last 20 years. Ann Surg. 2009;249(1):63–71.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 99.
Comment
Thickened folds and spasm of the duodenal bulb and sweep can be seen in a number of conditions both primary in the duodenum or in the adjacent structures in the periduodenal area. In the duodenum the commonest is the result of peptic ulcer disease. Although spasm is not always a component, thickened fold can be seen in such conditions as Zollinger-Ellison syndrome, eosinophilic enteritis, Crohn’s disease, Whipple’s disease, and amyloid, as well as intramural bleeding and hypoproteinemia. Also to be considered are malignancies.
Pancreatitis affecting the pancreatic head almost always affects the folds of the second portion of the duodenum (see figures). The folds appear thick and irregular, especially on the pancreatic side (see figures). There may be tethering of folds (Selleck’s folds), also seen on the same side (see figures).
The most common primary malignancy of the duodenum is adenocarcinoma, which accounts for 64% of tumors. The distribution of other primary tumors comprises carcinoid, 21%; lymphoma, 10%; and sarcoma, 4%. Elsewhere in the small bowel, the proportion of patients with carcinoids has increased, and carcinoid is now the most common tumor in the ileum. Sarcomas and lymphomas can develop throughout the entire small bowel.
Besides the pancreas, the right kidney bears a close and, in many patients, a contiguous relationship to the duodenum. It is not unusual to see a large right-sided upper pole renal malignancy affecting the adjacent duodenum.






