CASE 178
History: A 19-year-old man presents with weight loss and abdominal distention.
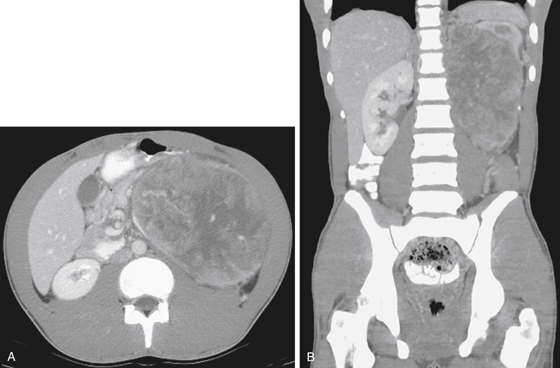
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. Which of the following statements regarding Wilms’ tumor is true?
A. Almost all Wilms’ tumors are solitary lesions.
B. Age at presentation is most commonly 5 to 10 years.
C. The tumor is typically well defined, surrounded by a pseudocapsule.
D. Children with associated congenital abnormalities usually present later.
3. Which of the following statements regarding renal cell carcinoma (RCC) is true?
A. Tumor calcification usually forms a thin peripheral rim.
B. Most patients present with hematuria, flank pain, and a palpable abdominal mass.
C. Multifocal RCCs are most commonly associated with acquired cystic disease of dialysis.
D. On contrast-enhanced CT scan, RCCs are most conspicuous on nephrographic phase imaging.
4. Which of the following statements regarding renal tumors is false?
B. Lymphoma involving the kidney most commonly occurs as multiple low-attenuation lesions.
C. Metastatic disease to the kidneys is the most common renal malignancy.
D. Oncocytomas are the most commonly excised benign solid renal tumor.
ANSWERS
CASE 178
Recurrent Wilms’ Tumor
1. A, B, and D
2. C
3. D
4. A
References
Dyer R, DiSantis DJ, McClennan BL. Simplified imaging approach for evaluation of the solid renal mass in adults. Radiology. 2008;247(2):331-343.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 59.
Comment
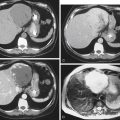
Wilms’ tumor is a solid tumor arising from the kidney that is seen in children and infants. It is the fifth most common cancer in children. It is diagnosed and treated in childhood. Wilms’ tumor is currently a treatable and curable condition. Almost 90% of patients survive 5 years after diagnosis as opposed to the poor prognosis of 25 years ago. In this case, the patient had Wilms’ tumor of early childhood that was successfully treated. Almost 15 years later, the tumor has recurred, as these tumors are known to do (2% to 3% after nephrectomy) with a much reduced survival rate (20% to 40%).
This tumor falls into the category of large extrinsic masses affecting the bowel (see figures). In the left upper quadrant, splenomegaly, pancreatic pseudocysts, pancreatic masses, subphrenic processes or processes relating to the proximal jejunum, and splenic flexure of the colon would be considerations. In a young patient with a large abdominal mass, the question of recurrent childhood tumor would be raised. Such recurrence is unusual but does occur. Most of the extrinsic processes mentioned compress or displace the adjacent bowel. Rarely, there may be contiguous invasion. In this case, the stomach can be seen sandwiched between the diaphragm and the tumorous mass without local invasion.