CASE 177
History: A 47-year-old man with long-standing dysphagia and recurrent pneumonia has developed hemoptysis.
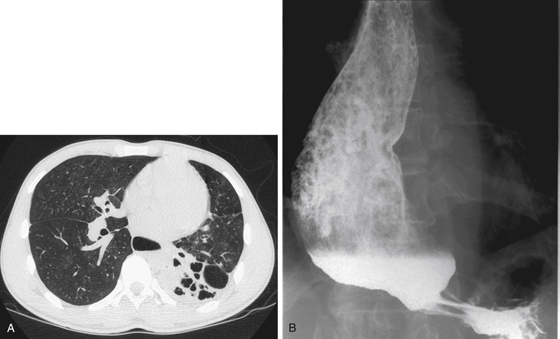
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
E. Gastroesophageal junction cancer
2. What is the underlying pathophysiologic defect in achalasia?
3. Which of the following conditions is associated with the highest risk of developing esophageal carcinoma?
4. Which of the following statements regarding conditions predisposing to esophageal cancer is true?
A. In achalasia, cancer develops as a result of chronic stasis.
B. Carcinoma developing in a lye stricture has a more dismal prognosis.
C. The Northern Asia cluster of esophageal carcinoma is due to Epstein-Barr virus.
ANSWERS
CASE 177
Esophageal Carcinoma Developing in Achalasia
1. A, B, C, and E
2. D
3. A
4. A
References
Leeuwenburgh I, Scholten P, Alderliesten J, et al: Long-term esophageal cancer risk in patients with primary achalasia: a prospective study. Am J Gastroenterol. 2010;105(10):2144-2149.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 21.
Comment
Achalasia is a common but poorly understood disorder of esophageal motility, producing lifelong dysfunction. It is a neurogenic disorder marked by a decrease or absence of ganglion cells in the esophagus. Abnormalities also have been found in the vagal trunks and nuclei. The underlying etiology for this loss of innervation is uncertain. The result is decreasing esophageal peristalsis and failure of the lower esophageal sphincter to relax. Achalasia occurs almost equally among men and women. Onset is typically in early adulthood, and later onset should raise suspicions of carcinoma, which may mimic the condition (secondary achalasia). With long-standing achalasia, the esophagus becomes markedly dilated, and food is retained in it (see figures). Scleroderma, peptic strictures, and intramural spread of carcinoma at the gastroesophageal junction may produce a similar appearance.
An unusual complication of this condition is the development of esophageal carcinoma secondary to chronic stasis. This complication is said to affect approximately 5% of patients with achalasia, although there are many who believe the incidence to be much less. Some authors do not classify cancer as a complication of this condition and consider the prevalence of cancer in patients with achalasia no higher than in the general population. Achalasia is usually present 20 or more years before carcinoma is found. Typically, squamous cell carcinoma is present, but adenocarcinoma also has been reported.
Other conditions that have a proven association with an increased incidence of esophageal squamous carcinoma include lye strictures, head and neck tumors, celiac disease, Plummer-Vinson syndrome (Paterson-Kelly syndrome), radiation exposure, palmar and plantar hyperkeratosis, and skin conditions such as epidermolysis bullosa.






