CASE 174
History: A 47-year-old man presents with fever.
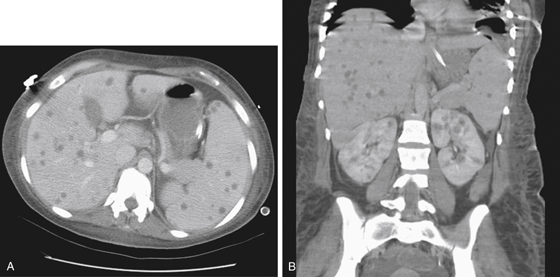
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
D. Echinococcus multilocularis
E. Multifocal cholangiocarcinoma
2. What is the most important predisposing factor to the development of hepatic microabscesses?
3. What is the most common causative organism of hepatic microabscesses?
4. Which of the following statements regarding liver infection is true?
A. The liver is the most common site of amebic infection.
B. On CT, the presence of calcified septa is pathognomonic of schistosomiasis.
C. Hydatid liver abscesses are most commonly due to E. multilocularis.
D. Acute miliary tuberculosis of the liver is characterized on CT by multiple tiny, dense nodules.
ANSWERS
CASE 174
Microabscesses of the Liver and Spleen
1. A, B, and C
2. B
3. A
4. B
References
Moore NJ, Leef JL, Pang Y. Systemic candidiasis. Radiographics. 2003;23(5):1287-1290.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 216.
Comment
Multiple low-density lesions throughout the liver or spleen may be the result of metastasis, which is the most common cause. However, when there are numerous tiny low-density areas occurring diffusely, the possibility of microabscesses must be seriously considered (see figures). The lesions almost always occur in the setting of some type of immunosuppression (e.g., patients with AIDS, transplant recipients, patients with leukemia, and patients with cancer undergoing chemotherapy). Patients receiving steroid therapy are another subgroup to be considered. The microabscesses develop as a result of systemic sepsis with a microorganism, usually fungal. However, many patients may have no irregular findings on blood cultures.
Candida albicans is the organism that most commonly produces this type of appearance. It is believed that this organism often resides in an immunosuppressed patient, and when the immune status of the patient decreases to a certain threshold, a systemic infection occurs. Other organisms that have been implicated include Cryptococcus and Aspergillus species. Rarely, this radiologic appearance can be attributed to some type of bacterial infection.
On ultrasound, these abscesses have a bright central echogenic focus with a surrounding hypoechoic band and “bull’s eye” lesion. Hepatic or splenic enlargement may be present. CT often reveals multiple low-density areas in the liver or spleen that often do not exceed 1 cm in diameter. Sometimes there is a central area of high density. Major differential considerations include metastases, and lymphoma may have a similar appearance.






