CHAPTER 17. RIGID SIGMOIDOSCOPY
The Corpus Hippocraticum of early medical works from ancient Greece described both proctoscopy and use of the rectal speculum, constituting the earliest published reference to endoscopy.
INTRODUCTION
Rigid sigmoidoscopy is a procedure that is usually performed in an out-patient setting. The transparent anoscope allows a 360 view of the anal canal and rectum, and hence has a significant role in the evaluation of anorectal and distal colonic pathology. This invasive procedure should be performed with care and sensitivity, maintaining the patient’s dignity at all times. This can only be learned after observing a senior colleague perform the procedure, and subsequently talking through the technique before performing it yourself under supervision.
INDICATIONS
• Symptoms or signs suggestive of anorectal or colonic pathology.
• As a routine investigation prior to anorectal procedures.
• Biopsy of anal canal.
• Removal of foreign bodies in the anal canal.
CONTRAINDICATIONS
Some of these are relative contraindications. The main concern is that of potential perforation.
EQUIPMENT
PRACTICAL PROCEDURE
 Tip Box
Tip Box
The bowels should be emptied pre-procedure with a glycerine suppository or phosphate enema.
• Explain the procedure and obtain consent.
• Set up the equipment on a clean trolley.
• Plug the equipment into the light source to ensure that it functions correctly.
• Position the patient into the left lateral decubitus (Sims’) position with the buttocks to the edge of the examination couch.
• Wash your hands, wear gloves and eye visor/goggles.
• Inspect the perineum and anus for evidence of fistulae, abscesses or skin tags.
• Go on to perform a digital rectal examination.
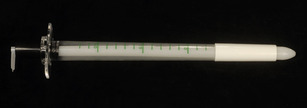
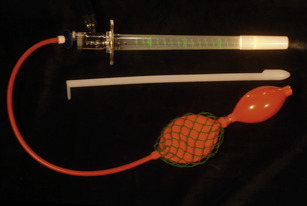
• Having completed the rectal examination, assemble the rigid obturator with the overlying plastic anoscope and apply lubricating gel.
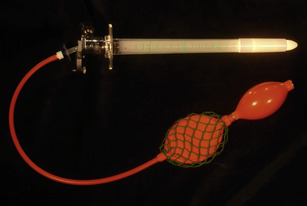
• Attach the non-disposable light-head (connected to mains) and bellows.
• Gently insert the lubricated device approximately 5 cm into the anus in the direction of the navel.
• Remove the obturator (Fig. 17.3).
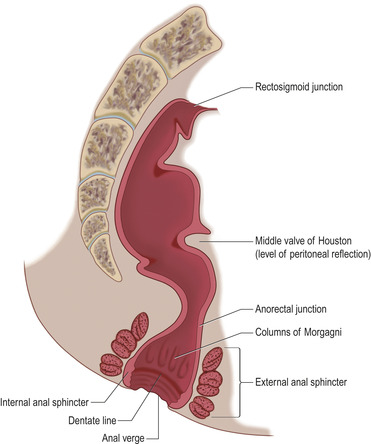
• Using the bellows of the rigid sigmoidoscope inflate a little air to open the anal canal and advance the sigmoidoscope further into the distal colon under direct vision up to 20 cm from the anal verge (Fig. 17.4).
 |
| Fig. 17.4 |
 |
| Fig. 17.5 |
• Having advanced to the required distance, slowly withdraw the rigid sigmoidoscope under direct vision, inspecting the bowel wall and the anal canal for fistulae openings, abscesses, fissures, internal haemorrhoids or neoplastic lesions.
 Tip Box
Tip Box
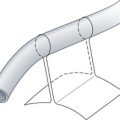
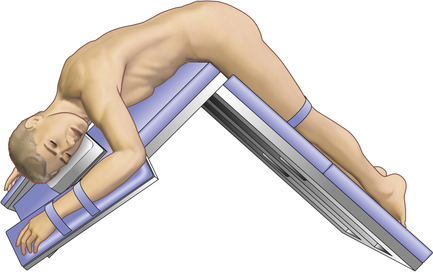
If either the patient experiences pain in the Sims’ position or you are unable to gain good views, try altering their position. The jack-knife position is an alternative that requires a special table that breaks in the middle (Fig. 17.5). Position the patient in a prone position on the table and secure them to the table with the straps. Lower the top of the table so the upper body and head are tilting downwards.
COMPLICATIONS
• Pain: should this occur, stop and remove the anoscope.
• Perforation.
• Infection.
• Haemorrhage.
• Localized bleeding.