CHAPTER 17 Case Studies
INTRODUCTION
The cases presented here illustrate two principles:
Quantitative Acupuncture Evaluation
The principle of QAE is discussed in detail in Chapter 6 and we provide only a summary here.
Quantitative evaluation is based on the following factors:
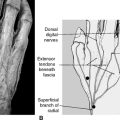
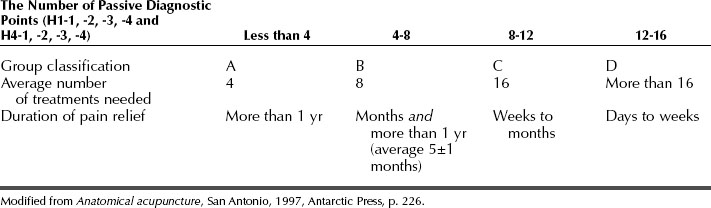
We selected 16 acupoints as evaluation points: palpating 4 points on the deep radial nerve on both arms and 4 points on the saphenous nerve on both legs enables us to divide patients into four groups: A, B, C, and D (Table 17-1).
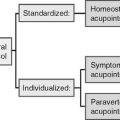
Standardized but Individualized INMAS Protocol
The INMAS treatment protocol ensures that every patient receives appropriately standardized treatment that is also adjusted to the patient’s personal condition. The INMAS protocol is described in detail in Chapter 5 and we provide only a summary here.
The principles of quantitative evaluation and individualization of the standardized INMAS protocol are depicted in every case presented below. All of these cases involved real patients but their names have been changed to protect their privacy.
NECK AND BACK PAIN
Group A: Excellent Results
Case 2: Lower Back and Neck Pain
AB is fit and healthy and has no previous physical injuries. Quantitative evaluation placed him in group A. Visual examination showed that his left shoulder was higher than his right. Upon palpation, acupoints on the left of the neck and the left shoulder area (H7, H3, H13, and H8) were more tender than acupoints on the right side. Left lumbar acupoints (H14, H15, and H16) were sore upon palpation. The impression was that the pain in the lower back and neck was of an acute nature. The prognosis was that pain relief could be achieved within four treatments.
Treatment Plan
Treatment Plan
The treatments were administered in the prone position. The acupoints selected were:
Group B: Good Results
Treatment Plan
Treatments were administered in the prone position. The selected acupoints were:
Case 7: Lower Back Pain
BG had no previous medical problems. Quantitative evaluation placed him in group B. Upon palpation, his left lumbar muscles were more sensitive than those on the right, and the left lumbar acupoints (H15, H14, H22, and H16) were tender, especially H22. The neck area was healthy, without any tender points. Given the foregoing, treatments were concentrated on the lower back. The back pain was treatable because of its acute nature. The prognosis was that about eight treatments should be enough to reduce the present pain and, given 30-years-worth of lower back stiffness, about four more treatments would be needed to prevent lower back pain in the future. Thus, the prognosis was that initially eight treatments would be necessary.
Treatment Plan
Treatments were administered in the prone position. The acupoints selected were:
Treatment Plan
Treatments were administered in the prone position. The acupoints selected were:
Treatment Plan
Treatments were administered in the prone position. The acupoints selected were:
Treatment Plan
Treatments were administered in the prone position. The acupoints selected were:
Group C: Average Results
Treatment Plan
Treatments were administered in the prone position. The acupoints selected were:
Treatment Plan
Group D: Low Responders
Treatment Plan
Treatments were administered in the prone position. The acupoints selected were:
Case 15: Lower Back Pain
We used the INMAS protocol with minor adjustment of the SAs according to his pain during every session. KK received two treatments a week for the first 2 weeks, then one session a week. He felt some improvement after each treatment, but the pain would come back the following day. After the eighth session, KK decided to stop acupuncture treatment and to have another surgery.
NECK AND UPPER LIMB PAIN
Treatment Plan Prone position.
Treatment Plan
Prone position. The acupoints selected were:
Supine position. The acupoints selected were:
Treatment Plan
HIP, LOWER LIMB AND FOOT PAIN.
Case 20: Foot Fasciitis
ST is healthy and used to be athletic, but could not exercise since the foot problem. Qualitative analysis placed ST in group A. Palpation showed that the pain might have been caused by an inflammation of the plantar fascia (fasciitis). To supplement the acupuncture treatments, we suggested that ST wear an orthopedic shoe as often as possible. Considering the prior surgical intervention, the prognosis was that 8 to 12 treatments would be needed.
Treatment Plan
Treatments were administered in the prone position. The acupoints selected were:
Treatment Plan
Treatments were administered in the prone position. The acupoints selected were:
Treatment Plan
Prone position. The acupoints selected were:
Treatment Plan
Prone position. The acupoints selected were:
Supine position. The acupoints selected were:
SHINGLES
Treatment Plan
Treatments were administered with the patient lying on her right side. The acupoints selected were:
HEADACHE
Treatment Plan
Treatments were administered in the prone position. The acupoints selected were:
Case 27: Headache
Quantitative evaluation placed CC in group C. Upon palpation, tender acupoints were found around every HA. We believed that her headache was related to her homeostatic condition and suggested that she drink fresh vegetable juice several times a day to cure the constipation. Our prognosis was that she needed 2 to 3 months of acupuncture treatments.
Treatment Plan
Prone position. The acupoints selected were:
NON-PAIN SYMPTOMS
Case 28: Bell’s Palsy (1)
RS is healthy and exercises in a gym everyday. He has no previous medical problems.
Treatment Plan
Prone position. The acupoints selected were:
Supine position. The acupoints selected were:
Case 29: Bell’s Palsy (2)
AS, a 65-year-old woman, came to the clinic with Bell’s palsy. She retired from her job in a bank 5 years previously. She started to have shingles on the left foot, leg, and hip. One month later, in the morning, she suddenly felt paralysis on the left side of the face. She was told that the paralysis would resolve itself in a few days. She waited for 2 months and still did not experience any improvement.
Treatment Plan
Prone position. Acupoints selected were:
Treatment Plan
Prone position. The acupoints selected were:
Supine position. The acupoints selected were:
The treatment plan was repeated once every day for 2 days. Most skin wheals subsided after the third treatment except the skin on the medial sides of the thigh and on the cubital fossa. After the third treatment the same needling was repeated with the addition of 5 to 10 needles inserted into the itchy skin on the medial thighs and cubital fossae. After the fifth treatment, the skin completely cleared up and the itching stopped.
Neurodermatitis can be treated in the same way. Apply needles to the following acupoints: