CASE 168
History: A 24-year-old man presents with fever and abdominal pain and distention.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the cause for the high-density focus within this abnormality shown in figure 2? (Hint: The plain radiograph shown in Figure C may be helpful.)
3. Why is it radiopaque?
4. What treatment may be performed by the radiologist?
A. Angiography and embolization
ANSWERS
CASE 168
Gossypiboma (Retained Surgical Sponge and Abscess)
1. A, B, C, and E
2. B
3. C
4. C
References
Hunter TB, Taljanovic MS. Medical devices of the abdomen and pelvis. Radiographics. 2005;25(2):503–523.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 318.
Comment
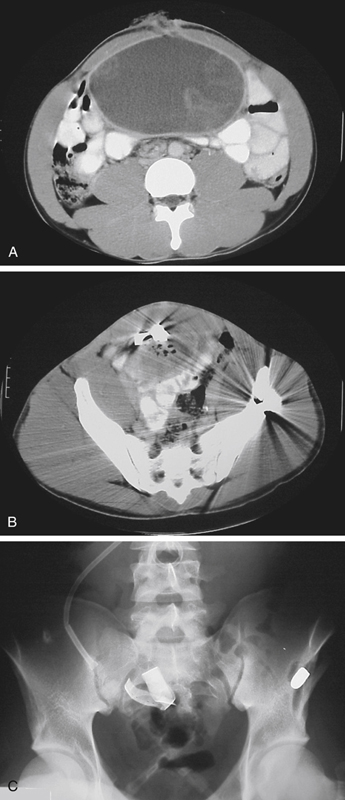
This CT scan shows an abnormal collection of mainly fluid and traces of gas within the anterior abdomen consistent with an abscess (see figures). Of greater importance, however, is the presence of a ribbonlike density within the abscess, which is indicative of some type of foreign object within the abdominal cavity (see figures). It can be seen distinctly on the plain image of the abdomen (see figures). This constellation of findings along with a history of prior abdominal surgery raises the likelihood of an iatrogenic cause (i.e., the introduction of some object into the peritoneal cavity during a surgical procedure). This object could be a surgical sponge or towel or perhaps a surgical needle that was dropped into the peritoneal cavity.
This complication is rare, considering the number of procedures performed daily. A retained surgical sponge (also known as a gossypiboma) can sometimes be difficult to diagnose. On plain film, motion artifact can make the radiopaque ribbon all but disappear. An intraoperative image obtained because of the possibility of a retained sponge must be obtained during complete suspended respiration. Motion artifact has been known to make the radiopaque ribbon virtually disappear. The radiopaque ribbon is placed in surgical sponges so that they can be identified on radiographs of the abdomen.
Intraoperative radiographs are obtained if the sponge count taken during surgery is incorrect. Radiography usually detects most sponges that are lost within the abdominal cavity. However, because of incorrect counting, the surgeon often may be unaware that a sponge has been lost within the abdominal cavity. Some of these objects produce no symptoms and are retained within the abdominal cavity until they are later discovered incidentally during a radiologic examination. Others may serve as a nidus for infection, leading to the development of an abscess, as in this patient. Surgery is the primary treatment when complications, such as abscess formation, occur as a result of a retained foreign object. However, in some instances, the abscess can be drained percutaneously if the patient is too ill for immediate surgery.






