CASE 167
History: An infant presents with a palpable lump under her chin.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the most common presentation of a thyroglossal duct cyst?
3. What is the most common complication of a thyroglossal duct cyst?
4. What is the definitive treatment of a thyroglossal duct cyst?
ANSWERS
CASE 167
Thyroglossal Cyst
1. A, B, C, and D
2. B
3. B
4. A
References
Ahuja AT, Wong KT, King AD, et al: Imaging for thyroglossal duct cyst: the bare essentials. Clin Radiol. 2005;60(2):141–148.
Reede DL, Bergeron RT, Som PM. CT of thyroglossal duct cysts. Radiology. 1985;157(1):121–125.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 10.
Comment
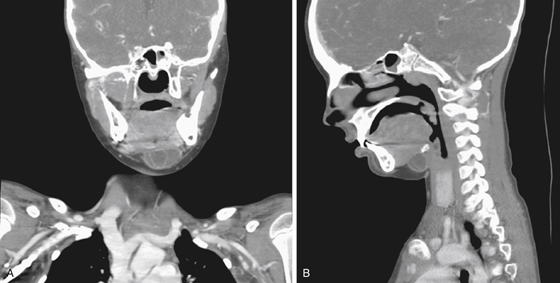
A thyroglossal cyst is a cystic structure formed in a persistent thyroglossal duct. This duct usually involutes early in embryonic life (8 to 9 weeks) but may retain some patency in a small percentage of the population, leading to cyst formation at the base of the tongue, often in the midline and occasionally touching the hyoid bone. Most patients are female and asymptomatic.
Occasionally, the cyst may cause a globus sensation or “dysphagia.” Barium swallow is usually normal. CT shows the mass at the base of the tongue, usually midline, but not always (see figures). It rarely exceeds 3 cm in size. Complications include infection, in which case the patient presents with painful swallowing (the cyst moves with the tongue) and a painful lump in the neck in a sublingual location. Rarely, an association of thyroglossal cyst with medullary carcinoma of the thyroid gland has been reported.
Other cystic structures in the neck or upper mediastinum to be considered are foregut cysts such as bronchogenic cysts, duplication cysts, neurogenic cysts, and thymic cysts. Many of these conditions produce no symptoms and are often incidental findings. However, as the individual ages, some of these cystic structures may become symptomatic.