CASE 166
History: A 39-year-old man presents with left lower quadrant pain of 4 days’ duration.
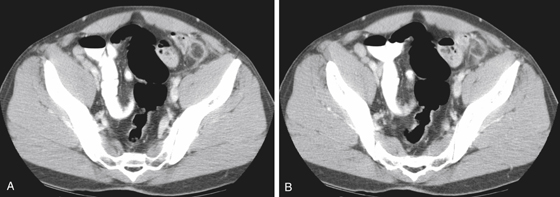
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the etiology of epiploic appendagitis?
A. Occlusion of the lumen of the appendage with debris
B. Bacterial contamination of the epiploic appendage
C. Torsion of the epiploic appendage
3. The lesion of epiploic appendagitis is described as an oval pericolonic lesion surrounded by inflammatory stranding. What is the density of this oval lesion?
4. What is the treatment for epiploic appendagitis?
ANSWERS
CASE 166
Epiploic Appendagitis
1. A, D, and E
2. C
3. A
4. A
References
Almeida AT, Melao L, Viamonte B, et al: Epiploic appendagitis: an entity frequently unknown to clinicians—diagnostic imaging, pitfalls, and look-alikes. AJR Am J Roentgenol. 2009;193(5):1243–1251.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 319.
Comment
Acute epiploic appendagitis is an unusual self-limiting inflammatory process involving the epiploic appendages of the colon. It is thought to be due to torsion of the appendage pedicle, which results in vascular occlusion, thrombus, and inflammation. The epiploic appendages are fatty extensions arising from the two rows of taeniae coli, which form the well-known haustral pattern of the colon. The taeniae are covered by peritoneum and are found anywhere along the length of the colon.
Before laparoscopy and CT, the condition went undiagnosed and the patient recovered, or it was mistaken for some other intraabdominal disease, and the patient underwent laparotomy. Multidetector CT is excellent not only for revealing the condition but also for excluding other causes of abdominal pain that might require immediate intervention. The treatment is conservative with spontaneous resolution in virtually all patients.
CT shows the inflamed appendage, as in this case, apart from the bowel wall and without inflammatory changes of the bowel wall (see figures). Follow-up CT scans may show involution with some scar tissue in the pericolonic fat. Tiny calcifications or focal fatty scarring in the fat around the pericolic regions may be indicative of prior epiploic appendagitis.