CASE 157
History: A 67-year-old man presents for evaluation of choking episodes.
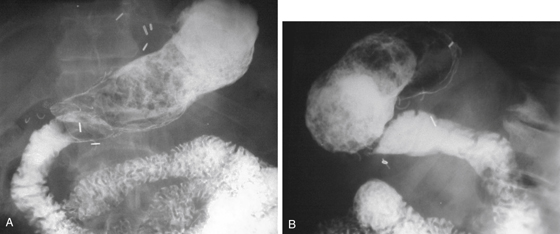
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. The stomach has an abnormal configuration as a result of previous surgery. What operation has been performed?
3. Which of the following is the most common material found in bezoars?
4. Which of the following postgastrectomy complications is more common after the Billroth II operation compared with the Billroth I operation?
ANSWERS
CASE 157
Gastric Bezoar in Post–Billroth I Stomach
1. A, B, and E
2. A
3. B
4. B
References
Ripolles T, Garcia-Aguayo J, Martinez M, et al: Gastrointestinal bezoars: sonographic and CT characteristics. AJR Am J Roentgenol. 2001;177(1):65–69.
Woodfield CA, Levine MS. The postoperative stomach. Eur J Radiol. 2005;53(3):341–352.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 78.
Comment
Gastric bezoars represent a complication of gastric surgery relating to disordered motility. However, bezoars can be seen in stomachs with normal anatomy as well. A bezoar is a ball of foreign or nondigestible material that does not pass the pylorus or the stoma in a postoperative stomach (see figures). Most bezoars are seen as a complication of gastric surgery or as the result of the ingestion of nonfood items, such as hair (trichobezoars) or indigestible fiber (phytobezoars). The fruit of the persimmon tree is almost always used as an example and is probably the most common cause of bezoars in nonsurgical stomachs in the United States. Bezoars have been reported with other accumulations of fiber in the stomach as well, including psyllium fiber powder laxatives ingested with insufficient water.
After gastric surgery, the occurrence of bezoars is thought to range from 5% to 12%; this can seem high given day-to-day experience with these patients. Such indigestible items as orange peels, potato peels, and laxative fiber probably account for most bezoars in this setting. Bilateral vagotomy, which usually accompanies gastric resection, leading to the resultant alteration in gastric emptying, is largely the source of the problem.
After gastric surgery, patients with a gastric bezoar often complain of abdominal discomfort, pain, fullness, and vomiting. Rarely, bezoars can occur in other parts of the gastrointestinal tract. Also found in the literature are reports of unusual types of bezoars such as varnish bezoars in detail painters for fine furniture.






