CASE 157



1. What should be included in the differential diagnosis? (Choose all that apply.)
A. Aorta
B. Renal artery
3. If this patient has pain in the temples and double vision, what is the most likely diagnosis?
4. What is the best way to confirm the diagnosis?
B. Erythrocyte sedimentation rate
C. MRI
ANSWERS
References
Borchers AT, Gershwin ME. Giant cell arteritis: a review of classification, pathophysiology, geoepidemiology and treatment. Autoimmun Rev. 2012;11(6–7):A544–A554.
Katabathina VS, Restrepo CS. Infectious and noninfectious aortitis: cross-sectional imaging findings. Semin Ultrasound CT MR. 2012;33(3):207–221.
Reddy GP, Gunn M, Mitsumori LM, et al. Multislice CT and MRI of the thoracic aorta. In: Webb WR, Higgins CB, eds. Thoracic imaging: pulmonary and cardiovascular radiology. ed 2 Philadelphia: Lippincott Williams & Wilkins; 2010.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, p 398.
Comment
Clinical Features
Giant cell arteritis (synonyms include temporal or cranial arteritis) is a systemic granulomatous panarteritis. It is classically associated with temporal and cranial arteries, but it involves other vessels, including the aorta, coronary arteries, and mesenteric arteries. Patients can present with systemic symptoms such as fatigue or with more specific symptoms such as temporal pain, scalp tenderness, headaches, and vision disturbance. Giant cell arteritis occurs almost exclusively in patients older than 50 and is closely associated with polymyalgia rheumatica (i.e., pain and stiffness in the muscles of the pelvis and shoulders).
Diagnosis
On physical examination, temporal arteries can be hard, and the temporal pulse can be weak. Systemic inflammatory blood markers (e.g., erythrocyte sedimentation rate and C-reactive protein) are generally elevated. Temporal artery biopsy establishes the diagnosis. Prompt administration of high-dose corticosteroids is the treatment of choice because this disease is associated with sudden-onset blindness.
Imaging
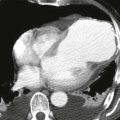
MRI and CT can show dilation or stenosis of the arteries and wall thickening (Figs. A–C). MRI can show enhancement of the arterial wall or high T2 signal indicating edema. Aortic involvement is seen in about 15% of all cases of giant cell arteritis. Aortic complications seen with giant cell arteritis include aortic dissection, aortic regurgitation, and abdominal or thoracic aortic aneurysms. FDG-PET is sensitive in diagnosing active inflammation in extracranial arteries. Clinical features and patient age help differentiate giant cell arteritis from Takayasu arteritis.