CASE 155
History: A 25-year-old woman presents with sudden onset of severe abdominal pain after several episodes of intermittent abdominal pain and swelling.
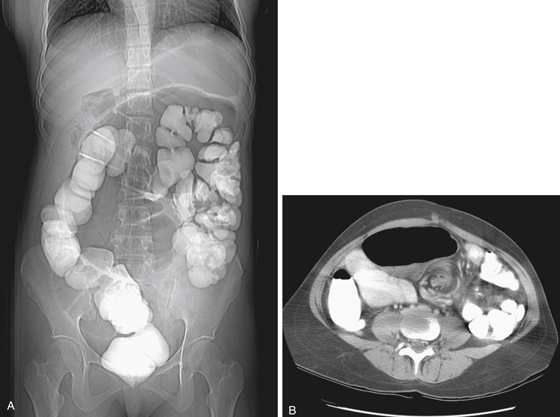
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What name best describes the type of obstruction that results in the marked dilation seen in this case?
3. In what age group is this condition of mesenteric volvulus most commonly seen?
4. What imaging examination would you consider next?
ANSWERS
CASE 155
Mesenteric Volvulus
1. A, B, and C
2. C
3. B
4. A
References
Peterson CM, Anderson JS, Hara AK, et al: Volvulus of the gastrointestinal tract: appearances at multi-modality imaging. Radiographics. 2009;29(5):1281–1293.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 110.
Comment
Small bowel, or mesenteric, volvulus is a life-threatening condition that occurs when a loop or loops of small bowel twist around its mesenteric root. When complete occlusion occurs, it is, in effect, a “closed-loop obstruction” and requires immediate treatment to avoid compromise of the vascular pedicle, bowel necrosis, perforation, peritonitis, and death. The condition may be transitory in some cases. However, even when the bowel is unobstructed, CT may suggest the possibility of the diagnosis by the swirling appearance of the root of the mesentery, even if the patient is unobstructed. In this case, the swirling configuration of the mesenteric root is quite pronounced, and the patient is experiencing a closed-loop obstruction with gross dilation of loops of small bowel in the midabdomen (see figures).
The condition is most frequently seen in infants with midgut malrotation, Ladd’s bands, and the attendant increase risk of midgut volvulus. This condition is sometimes referred to as secondary mesenteric volvulus because there are underlying congenital causes for the volvulus. However, mesenteric volvulus is occasionally seen in older individuals as a primary volvulus in which no congenital abnormalities are present. Conditions such as an extra long mesentery, high-fiber diet, or anorexia may contribute to the development of the condition; however, this is speculation and it is unknown why some patients develop this condition.
Mesenteric volvulus is uncommon and represents about 1% to 2% of small bowel obstructions. However, a full-blown twist of the mesenteric root and the resulting closed-loop obstruction can lead to mesenteric infarction in almost half of patients. There is probably a direct correlation of morbidity to the length of the interval between diagnosis and treatment.
Not all swirling seen at the mesenteric root is a small bowel volvulus. As indicated, it may be a transient process that results in complicated work-ups without significant results. Similar to cases of transient intussusception, seeing the patient between episodes can be problematic.






