CASE 154
History: A 54-year-old woman presents with abdominal pain.
1. What should be included in the differential diagnosis of the imaging finding shown in the figure? (Choose all that apply.)
2. What is the peritoneal space posterior to the stomach and anterior to the pancreas called?
3. Which of the following is the viscus most commonly herniated through the foramen of Winslow?
4. Which of the following is the most common of the various internal hernias?
ANSWERS
CASE 154
Foramen of Winslow Internal Bowel Hernia
1. A, C, and E
2. A
3. B
4. B
References
Martin LC, Merkle EM, Thompson WM. Review of internal hernias: radiographic and clinical findings. AJR Am J Roentgenol. 2006;186(3):703–717.
Takeyama N, Gokan T, Ohgiya Y, et al: CT of internal hernias. Radiographics. 2005;25(4):997–1015.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 331.
Comment
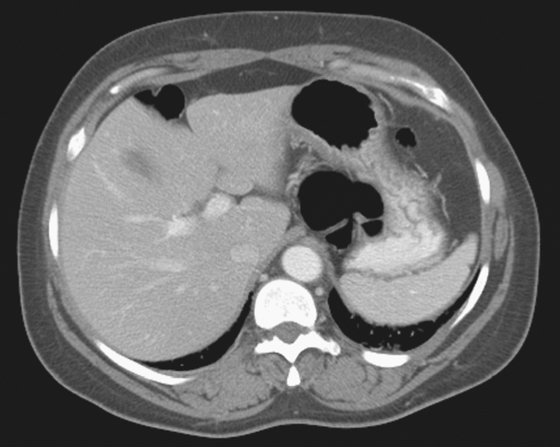
The foramen of Winslow (also known as the epiploic foramen) lies at the right free edge of the hepatogastric and hepatoduodenal ligaments in the region of the underside of the liver. It is posterior to the edge of the lesser omentum, just to the right of the spine. It is normally a little larger than the width of a finger but can be much larger in some people. It is unusual to see bowel herniation via the foramen into the lesser sac. The clinician must take time to evaluate carefully because a right paraduodenal hernia can have a similar appearance. If the herniated bowel crosses the midline to the right, it is evidence of a hernia of the foramen of Winslow. In some cases, such as this case, it is redundant transverse colon or right colon with little or no retroperitonization that herniates through the foramen. If the bowel becomes strangulated, it becomes a surgical emergency.
A barium enema would be very helpful, but as seen in this case, CT suggests the diagnosis (see figure). On plain film, the gastric air bubble is seen along with a collection of air overlying but not in the stomach. On this CT image, air is seen behind the stomach in the region of the gastrohepatic ligament and the foramen itself.
Internal bowel hernias are uncommon, and hernias of the foramen of Winslow are even less common. Most internal hernias are paraduodenal or transmesenteric. Many hernias are asymptomatic and are discovered incidentally. The hernia can also be transient and be the cause of endless work-ups for a patient with vague abdominal complaints and transient obstructive symptoms. It is also possible for the herniated bowel to compress the common bile duct, and a few cases of jaundice relating to hernias of the foramen of Winslow have been reported.






