[level-membership-for-cardiovascular-category]
CASE 154

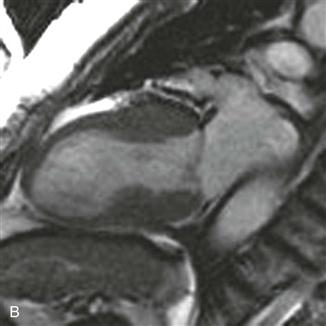
1. What should be included in the differential diagnosis based on the history and the steady-state free precession (SSFP) images (Figs. A and B)? (Choose all that apply.)
B. Noncompaction cardiomyopathy
D. Hypertrophic cardiomyopathy
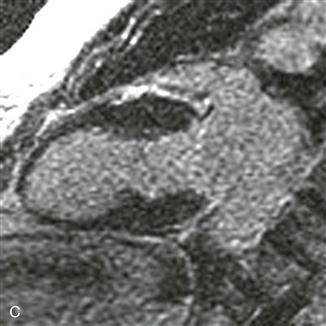
2. What does the late gadolinium enhancement image show?
A. No late gadolinium enhancement
B. Midmyocardial late gadolinium enhancement
C. Subendocardial late gadolinium enhancement
D. Transmural late gadolinium enhancement
3. Based on the history and the figures, what is the most likely diagnosis?
B. Noncompaction cardiomyopathy
D. Hypertrophic cardiomyopathy
4. Which imaging plane was used in these sequences?
A. Short axis
ANSWERS
References
Fernández-Pérez GC, Aguilar-Arjona JA, de la Fuente GT, et al. Takotsubo cardiomyopathy: assessment with cardiac MRI. AJR Am J Roentgenol. 2010;195(2):W139–W145.
Neil CJ, Nguyen TH, Sverdlov AL, et al. Can we make sense of takotsubo cardiomyopathy? An update on pathogenesis, diagnosis and natural history. Expert Rev Cardiovasc Ther. 2012;10(2):215–221.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 294–295.
Comment
Etiology and Clinical Features
Takotsubo cardiomyopathy, or stress cardiomyopathy (other synonyms include apical ballooning syndrome and broken-heart syndrome), is a reversible cardiac dysfunction brought on by extreme stress. Takotsubo cardiomyopathy typically affects postmenopausal women. Precipitating events include the death of a loved one, financial loss, or a breakup. Patients generally have new electrocardiogram changes (e.g., ST segment elevation or T wave inversion) and elevated cardiac enzyme biomarkers that mimic myocardial infarction. Symptoms also may overlap with symptoms of myocarditis. Treatment of Takotsubo cardiomyopathy is supportive; most patients fully recover left ventricular function within months of the initial presentation.
Imaging
Echocardiography, catheter-based ventriculography, and MRI can demonstrate dyskinesis or akinesis in the mid and apical left ventricle that spares the basal segments. The heart can take on an appearance similar to a takotsubo, a bulbous Japanese pot used to catch octopi. T2-weighted MRI can show increased signal intensity, consistent with edema, which does not correspond to a vascular distribution. In contrast to acute myocardial infarction, the hyperintense T2 signal and left ventricular contraction abnormality return to normal within a few weeks after the initial presentation (Figs. A and B). Late gadolinium enhancement images typically show no myocardial enhancement (Fig. C). To make the diagnosis, obstructive coronary artery disease, myocarditis, and pheochromocytoma should be excluded.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
CASE 154
1. What should be included in the differential diagnosis based on the history and the steady-state free precession (SSFP) images (Figs. A and B)? (Choose all that apply.)
B. Noncompaction cardiomyopathy
D. Hypertrophic cardiomyopathy
2. What does the late gadolinium enhancement image show?
A. No late gadolinium enhancement
B. Midmyocardial late gadolinium enhancement
C. Subendocardial late gadolinium enhancement
D. Transmural late gadolinium enhancement
[/not-level-membership-for-cardiovascular-category]
