CASE 153
1. What are possible distributions of hypertrophic cardiomyopathy (HCM)? (Choose all that apply.)
A. Septal
B. Concentric
D. Apical
2. What is the distribution of hypertrophy in this patient?
A. Septal
B. Concentric
D. Apical
3. Which country has the highest prevalence of apical HCM?
B. South Africa
C. Japan
D. Brazil
4. What is the etiology of HCM?
A. Sarcoidosis
B. Hypertension
C. Ischemia
D. Genetic
ANSWERS
Reference
Harris SR, Glockner J, Misselt AJ, et al. Cardiac MR imaging of nonischemic cardiomyopathies. Magn Reson Imaging Clin N Am. 2008;16(2):165–183.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 53, 284–288.
Comment
Etiology and Clinical Features
HCM is inherited as an autosomal dominant trait with variable penetrance. Patients have a variable clinical presentation; they may be asymptomatic, or they may have atrial fibrillation, heart failure, syncope, or sudden cardiac death, which is the leading cause of mortality in these patients. Asymmetric hypertrophy of the ventricular septum accounts for 90% of cases of HCM. Other patterns exhibit a right ventricular, left ventricular, septal, apical, midventricular, or concentric distribution. The apical pattern can account for 25% of patients in Japan, but it is uncommon elsewhere. Patients with heart failure secondary to significant hypertrophy can be treated with myectomy.
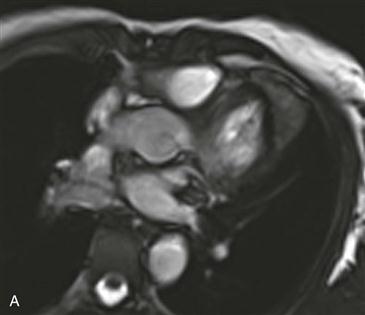
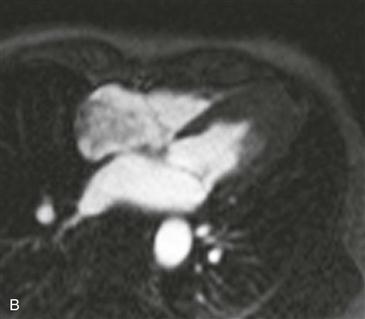
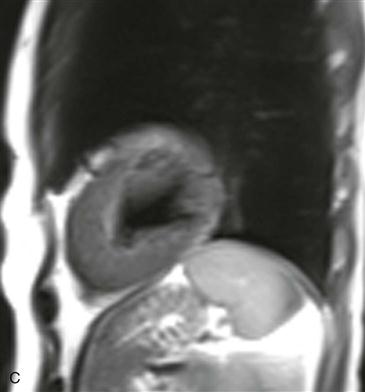
Imaging
MRI (Figs. A–C) can provide anatomic and functional information in HCM and can be most useful when the diagnosis is in question, when invasive therapy is being considered, or when clinical concern requires more thorough assessment than provided by echocardiography. MRI can be used to identify the distribution of thickened myocardium and to calculate left ventricular mass. Therapy may depend on the distribution of hypertrophy. MRI also can be used for functional evaluation of left ventricular outflow tract obstruction and myocardial perfusion and viability.






