CASE 152
History: A 42-year-old man presents with epigastric pain.
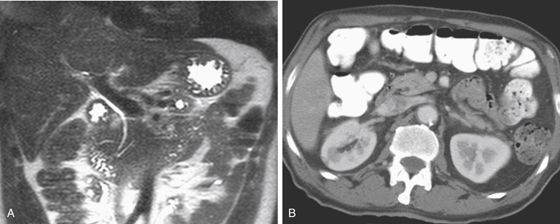
1. What is the diagnosis of the imaging finding shown in Figure A?
2. What is the most common congenital abnormality of the pancreatic gland and ducts?
3. What is the most common clinical scenario associated with pancreas divisum?
4. Pancreas divisum is characterized at endoscopic retrograde cholangiopancreatography (ERCP) by a duct in the head and uncinate of the pancreas with a foreshortened, arborizing appearance. What is the embryologic origin of this duct?
ANSWERS
CASE 152
Pancreas Divisum
1. B
2. B
3. A
4. B
References
Chalazonitis NA, Lachanis BS, Laspas F, et al: Pancreas divisum: magnetic resonance cholangiopancreatography findings. Singapore Med J. 2008;49(11):951–954.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 152.
Comment
The pancreas develops as two separate buds from the midgut that appear at about 5 weeks of gestation and fuse together shortly thereafter to form a single pancreas. Not only do the two buds fuse their tissue, but also the associated ductal structures must join. Because of the complex nature of the ductal structures, anomalies affecting the drainage of the pancreatic ducts occur in a large percentage of individuals. Embryologically, the major, or ventral, pancreatic bud develops into the ventral pancreas. In situations in which the ventral and dorsal buds do not fuse, as the ventral pancreas rotates, its duct becomes the major duct in the head of the pancreas with a foreshortened, arborizing appearance. It also is joined to the biliary system, and these ducts drain through the major papilla. The minor ventral bud of the pancreas develops separately and drains via the minor papilla. Under normal circumstances, the duct of Santorini fuses to the duct of Wirsung, and the Santorini duct goes on to drain through the Wirsung duct and into the major papilla. The portion of the Santorini duct that did drain into the duodenum usually involutes, and there is no separate papilla.
Pancreas divisum (seen in 4% to 7% of autopsy cases) may have several variations, the most common of which is when the less prominent ventral duct maintains its separate drainage, along with the bile duct, into the duodenum via the major papilla. The minor papilla is usually proximal to the major papilla and drains the greater dorsal duct. The dorsal duct drains the body and tail, and the ventral duct drains the head and uncinate. In some instances, as in this case, there may be a tiny communicating branch between the two systems.
Most cases of pancreas divisum are discovered incidentally during ERCP or, as in this case (see figures), magnetic resonance cholangiopancreatography (MRCP). However, there is a higher than normal incidence of pancreatitis in these patients. The exact etiology of pancreatitis in pancreatic divisum, excluding all other factors (e.g., stones, alcohol), is unclear. Some researchers think it relates to the major duct attempting to empty its exocrine content into the duodenum via a tiny minor papilla. Acute pancreatitis in a young person should arouse some suspicion for this condition. Although ERCP or MRCP would be the examination of choice, a CT scan showing what appears to be three ducts in the pancreatic head is suggestive, as in the CT image of this case (see figures).






