CASE 151

1. What abnormalities can cause a pulsatile mass at the base of the neck? (Choose all that apply.)
C. Right subclavian artery aneurysm
D. Aneurysm of right aortic arch
2. Which pharyngeal arch forms the normal aortic arch?
A. Third
B. Fourth
C. Fifth
D. Sixth
3. The right third pharyngeal arch can form which anomaly?
C. Left arch with aberrant right subclavian artery
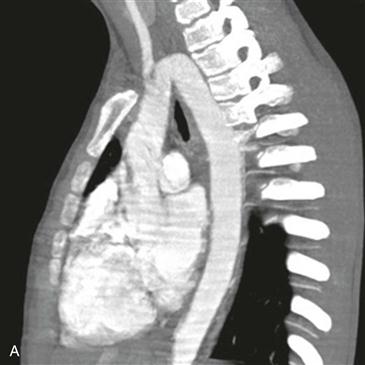
4. Based on the CT scan, what is the most likely diagnosis?
ANSWERS
References
Caputo S, Villanacci R, Ciampi Q, et al. Cervical aortic arch: echocardiographic and three-dimensional computed tomography view. Echocardiography. 2010;27(4):E44–E45.
Poellinger A, Lembcke AE, Elgeti T, et al. Images in cardiovascular medicine The cervical aortic arch: a rare vascular anomaly. Circulation. 2008;117(20):2716–2717.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, p 427.
Comment
Etiology and Clinical Features
Cervical aortic arch is a rare anomaly in which the arch arises from the primitive third arch instead of the fourth arch. It may be more common on the right side. It has been reported that the ipsilateral internal and external carotid and vertebral arteries arise directly from the arch. Cervical aortic arch is usually asymptomatic but can manifest as a pulsatile mass in the supraclavicular fossa or neck, with obstruction from kinking, or as an aneurysm. Other symptoms include stridor, frequent respiratory infections, and dyspnea on exertion. Patients with cervical aortic arch do not require treatment unless there is an aneurysm or respiratory symptoms.
Imaging and Diagnosis
Diagnosis is based on the presence of the aortic arch near the base of the neck. Some authors state that the diagnosis depends on the finding of separate origins of the internal and external carotid arteries directly from the arch. MRI and CT delineate the anatomy (Figs. A and B). A cervical aortic arch extends above the level of the clavicles and manubrium and may extend to the C2 vertebral body.






