CASE 150
History: A 32-year-old woman presents with abdominal pain.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What finding on MRI most reflects active pathologic inflammation of the bowel in Crohn’s disease?
3. What is the main advantage of MRI over CT for the evaluation of Crohn’s disease?
D. Improved spatial resolution
4. In this case, small bowel feces has occurred secondary to Crohn’s disease. With which of the following conditions would you not expect small bowel feces to occur?
ANSWERS
CASE 150
Small Bowel Feces Sign in Crohn’s Disease
1. B, C, and E
2. C
3. C
4. D
References
Sempere GA, Martinez Sanjuan V, Medina Chulia E, et al: MRI evaluation of inflammatory activity in Crohn’s disease. AJR Am J Roentgenol. 2005;184(6):1829–1835.
Wills JS, Lobis IF, Denstman FJ. Crohn disease: state of the art. Radiology. 1997;202(3):597–610.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 137.
Comment
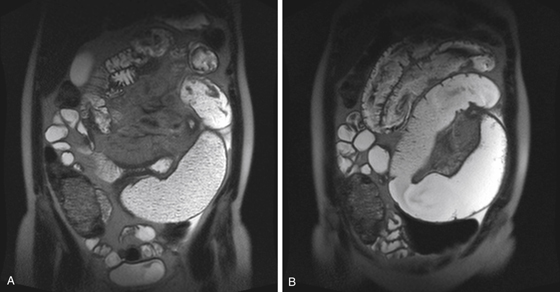
Despite its appearance, what looks like stool in the loop of bowel is actually fecal-like material backed up behind a stricture in the ileum of a young woman with Crohn’s disease. Note the thickened inflamed bowel and a stricture with proximal dilation and feces-like material distending the loop of obstructed small bowel (see figures). This finding, the small bowel feces sign (SBFS), although not rare, is relatively uncommon. It is most likely to occur in patients with long-standing moderate to severe narrowing of the small bowel. SBFS is often seen in patients with Crohn’s disease. However, it has also been described in patients with small bowel obstruction secondary to adhesions, ischemia, hernias, and cystic fibrosis.
Any chronic, slow-developing obstruction may result in this finding. The SBFS is helpful in that it occurs at the level of the obstruction, with the distal tip of the feces-like material tapering down to the exact obstructive site. Generally, CT is a fast and effective way to evaluate for potential small bowel or even colonic obstruction. It can be done quickly without luminal contrast because dilated bowel proximal to the obstructing site is usually distended with air or, more likely, fluid. The identification of normal-caliber bowel and its relationship to fluid-filled distended bowel can often detect the obstructing site and, in some cases, the offending agent. Adhesions are difficult to see with CT; the absence of any other cause of a sudden transition is suggestive of adhesions. Because adhesions are the most common cause of small bowel obstruction, and approximately 20% of hospital admissions are the result of some form of small bowel obstruction, CT evaluation is becoming an increasingly important diagnostic tool in these cases.






