CASE 15
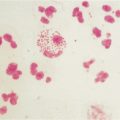
A 23-year-old woman, LL, is seen in your office complaining of flu-like symptoms that had persisted for several weeks. A physician at a local walk-in clinic gave her an antibiotic 2 weeks ago. She does not remember the name of it, but she finished the course of medications 3 days before coming to your office. She has noticed progressive pain in her hands and feet, and this morning on arising she noticed tender small bluish red spots on her fingertips. Your routine physical examination reveals nothing else of note. She is not a smoker, and she is currently afebrile. You order routine blood work and are called by the laboratory director when he noted the results indicated that she was profoundly anemic (see Appendix for reference values). At this stage you need to consider possible explanations for these findings; how might you investigate further?
QUESTIONS FOR GROUP DISCUSSION
RECOMMENDED APPROACH
Additional Laboratory Tests
Further laboratory investigation using the direct and indirect Coombs’ tests can be used to confirm (or rule out) drug-induced anemia as the cause of LL’s clinical presentation.
Coombs’ Tests
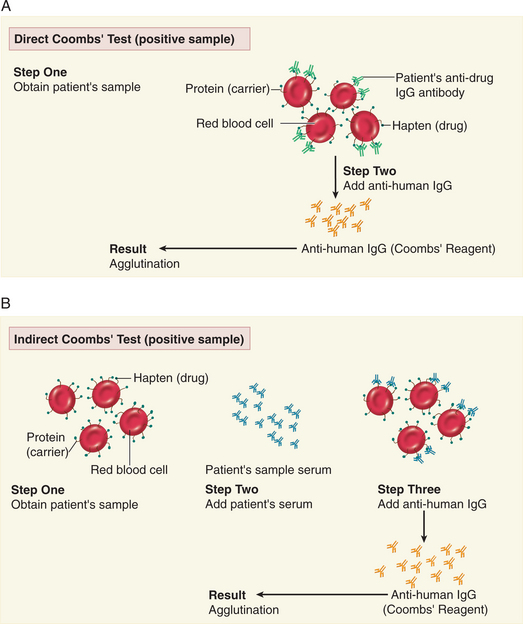
In the direct and indirect Coombs’ tests, a positive result is the visible manifestation of agglutination, resulting from aggregation and sedimentation of particulate antigen-antibody complexes (Fig. 15-1). In this case, the direct Coombs’ test was used to determine whether anti-drug IgG antibodies had formed and attached to drug/red blood cell complexes (Fig. 15-1A). The bound IgG antibodies are identified using anti-Fcγ antibodies generated in another species. When the anti-Fcγ antibodies crosslink anti-drug IgG antibodies, agglutination is observed and the sample is “positive.”
Indirect Coombs’ Tests
In contrast, in the indirect Coombs’ test we are testing for the presence of circulating anti-drug IgG antibodies in serum (see Fig. 15-1B). Therefore, an additional step is required before agglutination can be observed. This step is the incubation of LL’s serum with the red blood cells (to which we are assuming the drug has bound) to allow LL’s anti-drug antibodies (if present) to bind to the red blood cell complex. Thereafter, the test is the same as that described for the direct Coombs’ test. To determine the antibody titer, LL’s serum is serially diluted and the test is repeated. As the antibody concentration increases, agglutination will occur at higher and higher dilutions. Somewhat surprisingly to you, this test is negative!