[level-membership-for-gastroenterology-and-hepatology-category]CASE 148
History: A 72-year-old woman presents with abdominal distention and pain and tenderness in the right upper quadrant.
1. What should be included in the differential diagnosis of the imaging finding of the right lower quadrant calcification relevant to the abnormal appearance of the bowel shown in Figure A? (Choose all that apply.)
E. Mesenteric lymph node calcification
2. There are three radiographic features associated with gallstone ileus: an ectopic gallstone in the bowel, small bowel obstruction, and gas in the biliary system. What is the eponym for these signs?
3. In gallstone ileus, where does the stone most often impact itself?
4. Which statement regarding gallstone ileus is true?
A. Gallstone ileus causes 10% of cases of small bowel obstruction.
B. Gallstone ileus most commonly occurs in women older than 40 years.
D. Gallstone ileus occurs as a complication in 10% of patients with cholelithiasis.
ANSWERS
CASE 148
Gallstone Ileus
1. A and B
2. A
3. B
4. C
References
Lassandro F, Romano S, Ragozzino A, et al: Role of helical CT in diagnosis of gallstone ileus and related conditions. AJR Am J Roentgenol. 2005;185(5):1159–1165.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 136.
Comment
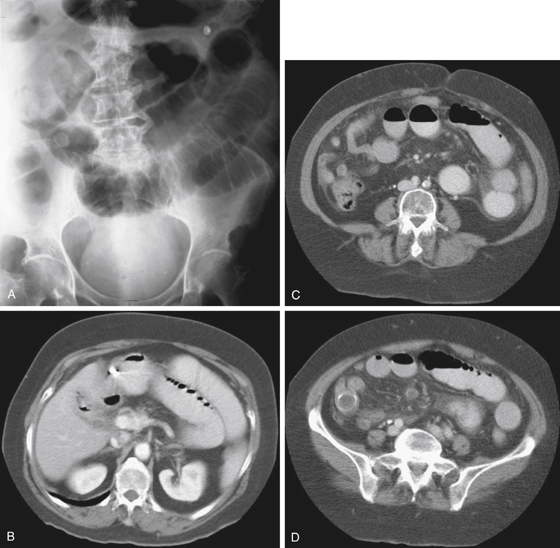
The term gallstone ileus refers to an unusual set of circumstances that develop in conjunction with chronic gallbladder disease and stone formation. In this condition, a large gallstone or gallstones develop. There must also be associated chronic cholecystitis. During this inflammation, a portion of the bowel becomes adherent to the gallbladder, which is a common occurrence in patients with chronic gallbladder inflammation. With time, the gallstone erodes through the gallbladder wall and into the lumen of the bowel, resulting in a cholecystenteric fistula. The fistula most commonly extends into the duodenum, but extension into the colon and the stomach also has been reported. As the large gallstone travels through the bowel lumen, it becomes impacted at a site where the lumen narrows, resulting in bowel dilation or obstruction.
The classic triad in this condition consists of gas in the biliary system, bowel obstruction, and a radiopaque stone evident in the abdomen (see figures). The biliary gas is seen in about 50% of cases and is secondary to the fistula that is open between the gallbladder and bowel. The amount of gas is often quite small. The stone is the most difficult finding to establish because of the bowel dilation. If it is not obscured by the contrast material, the stone often can be shown on CT (see figures). Finally, the bowel obstruction usually occurs in the terminal ileum at the ileocecal valve. Rarely, the stone obstructs the third portion of the duodenum, or the sigmoid colon. Infrequently (probably less than a third of the time), the entire triad of radiologic findings is present. Any time two of the entities are visible, the diagnosis of gallstone ileus should be considered.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 148
History: A 72-year-old woman presents with abdominal distention and pain and tenderness in the right upper quadrant.
1. What should be included in the differential diagnosis of the imaging finding of the right lower quadrant calcification relevant to the abnormal appearance of the bowel shown in Figure A? (Choose all that apply.)
E. Mesenteric lymph node calcification
2. There are three radiographic features associated with gallstone ileus: an ectopic gallstone in the bowel, small bowel obstruction, and gas in the biliary system. What is the eponym for these signs?
3. In gallstone ileus, where does the stone most often impact itself?
[/not-level-membership-for-gastroenterology-and-hepatology-category]
