CASE 146
History: A 73-year-old woman presents with lower abdominal pain.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
A. Fluid level in an ovarian dermoid
2. What is the most common etiology for a colovesical fistula?
3. What is the most common of the various fistulas of the lower urinary tract?
4. What is the most common cause of lower urinary tract fistulas?
ANSWERS
CASE 146
Colovesical Fistula
1. B, C, and D
2. D
3. C
4. C
References
Avritscher R, Madoff DC, Ramirez PT, et al: Fistulas of the lower urinary tract: percutaneous approaches for management of a difficult clinical entity. Radiographics. 2004;24(Suppl 1):S217–S236.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 316.
Comment
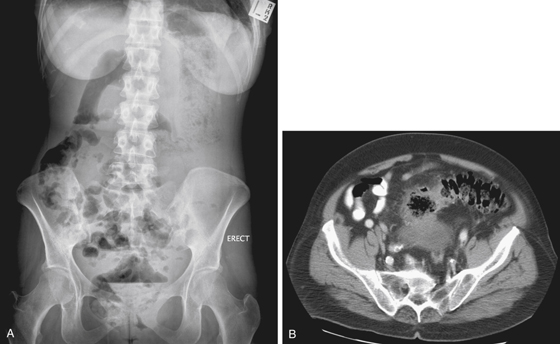
Of the many things to consider in radiologic evaluation of a plain image of the abdomen is the question, “Is there air in unexpected places?” In this case, allowing for exclusion of other innocuous causes such as bladder catheterization, air is seen in the urinary bladder (see figures) and must be considered abnormal, and a pathologic fistulous connection to an air-containing adjacent hollow organ viscus is a prime diagnostic consideration.
When considering the diagnosis, patient age and medical history become important. In a young patient, one might consider Crohn’s disease and possibly tuberculosis. If the patient has had a pelvic neoplasm treated with pelvic radiation, there is the possibility of a radiation-induced fistulous connection to bowel. Older patients would be more likely to have colonic diverticulitis as the underlying process. From the plain film, it is not difficult to ascertain that this is an older patient (73-year-old woman). The transaxial image confirms pericolonic inflammation with sigmoid diverticulitis as the underlying cause. The paracolic abscess pointed to and connected with the bladder (see figures). With the naturally occurring abscess drainage, the patient reported feeling better, but she experienced pneumaturia.






