[level-membership-for-cardiovascular-category]
CASE 146
1. What etiologies can cause this finding? (Choose all that apply.)
D. Tuberculosis
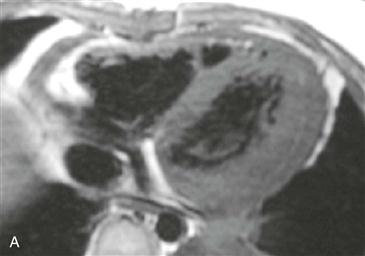
2. What is the pericardial abnormality in Fig. A?
A. Effusion
B. Thickening
D. Nodularity
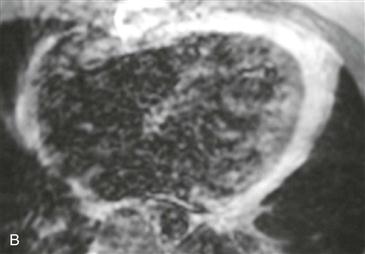
3. Given the symptoms and both images, what is the most likely diagnosis?
B. Inflammatory constrictive pericarditis
C. Effusive constrictive pericarditis
D. Tumor
4. What is the most appropriate treatment?
A. Antibiotics
ANSWERS
Reference
Wang ZJ, Reddy GP, Gotway MB, et al. CT and MR imaging of pericardial disease. Radiographics. 2003;23(Spec No):S167–S180.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 269–271.
Comment
Etiology and Physiology
Constrictive pericarditis occurs when limitation in diastolic ventricular filling leads to equalization of atrial and ventricular pressure, which is known as constrictive/restrictive physiology. Patients have symptoms similar to congestive heart failure. Physical examination may demonstrate the classic Kussmaul sign, which is the paradoxical elevation of jugular venous pressure on inspiration. Causes of constrictive pericarditis include open heart surgery, radiation therapy, uremic pericarditis, viral pericarditis, and tuberculous pericarditis (this is less common in industrialized countries).
Treatment
Constrictive pericarditis and restrictive cardiomyopathy have similar clinical presentations and findings on echocardiography and cardiac catheterization. However, it is important to differentiate between these two diseases because patients with constrictive disease usually benefit from pericardiectomy, whereas patients with restrictive cardiomyopathy have a poor prognosis and must be managed medically or with heart transplantation. Constrictive pericarditis, whether acute or chronic, can be treated by pericardial stripping.
Imaging
In the clinical setting of constrictive/restrictive physiology, pericardial thickening (≥4 mm) as demonstrated on MRI can establish the diagnosis of constrictive pericarditis (Figs. A and B). Pericardial thickening may be diffuse or localized to the right heart or atrioventricular grooves. Diastolic septal dysfunction (septal bounce) on cine MRI is another key finding. Ancillary findings may be present, including dilation of the inferior vena cava, hepatic veins, and right atrium, with a narrow, tubular right ventricle. It is important to remember that pericardial thickening can occur in the absence of constrictive physiology, and not all cases of surgically proven constrictive pericarditis have pericardial thickening. The diagnosis of constrictive pericarditis can be established only in the appropriate clinical setting of constrictive/restrictive physiology. Given the marked pericardial thickening and enhancement, the diagnosis of inflammatory constrictive pericarditis can be established.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
CASE 146
1. What etiologies can cause this finding? (Choose all that apply.)
D. Tuberculosis
2. What is the pericardial abnormality in Fig. A?
A. Effusion
B. Thickening
D. Nodularity
3. Given the symptoms and both images, what is the most likely diagnosis?
B. Inflammatory constrictive pericarditis
C. Effusive constrictive pericarditis
D. Tumor
[/not-level-membership-for-cardiovascular-category]
