CASE 144

History: A 61-year-old woman experiences acute pharyngeal pain during a meal of chicken.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
D. Calcified cervical osteophyte
E. Laryngeal cartilage calcification
2. In cases of suspected impacted pharyngeal chicken bone or other foreign body with inconclusive physical examination findings, what is the appropriate next step?
3. What is the most common site of impaction of an ingested foreign body?
4. After an impacted foreign body passes into the stomach, it usually continues through the intestinal tract without further hold-up. However, there are situations where endoscopic retrieval from the stomach is indicated. Which of the following is not such an indication?
ANSWERS
CASE 144
Chicken Bone Stuck at the Pharyngoesophageal Junction
1. A, B, C, and E
2. B
3. A
4. C
References
Low VHS, Killius JS. Animal, vegetable, or mineral: a collection of abdominal and alimentary foreign bodies. Appl Radiol. 2000;29:23–30.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 37.
Comment
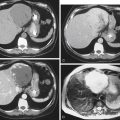
Fish or chicken bones caught in the cervical esophagus are a problem (1) because they are the most common foreign body seen in the upper esophagus, and (2) because they are among the hardest to see on routine imaging. The bones may not be radiopaque enough to see. There may be laryngeal calcifications that obscure them (see figures). Plain images of the neck have a low yield (approximately 20%). The contrast agent–soaked cotton pledgets employed before the advent of high-quality CT were virtually useless and a waste of time and radiation. I have been asked many times to do this examination for the suspicion of a fish or chicken bone lodged in the upper esophagus, and I have never seen a positive result. The idea was that the contrast agent–soaked pledget would hang up on the bone.
Plain images are still used as a screening tool, but ultimately the examination of choice is CT scan of the neck and upper esophagus. CT not only identifies the foreign body in almost every case but also assesses the area around the bone for penetration and complication. When a fish or chicken bone passes and is in the distal gastrointestinal tract, the problem is usually solved. However, the lodging and then passing of sharp objects may cause an abrasion of the upper esophageal mucosa. In these cases, the patient’s symptoms do not abate with the passing of the bone but may continue until the healing of the abrasion.