CASE 143
History: A 48-year-old woman presents with dysphagia and dyspepsia.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the most serious complication of partial gastrectomy?
3. What operation causes a gastric fundal pseudotumor?
D. Bilroth (1 or 2) operations
4. What is a pseudolymphoma of the stomach?
A. Thickened rugal folds secondary to varices
B. Gastric adenocarcinoma that resembles lymphoma
C. Lymphoid tissue proliferation that simulates lymphoma
D. Lymphoma developing from chronic Helicobacter gastritis
ANSWERS
CASE 143
Pseudotumor of the Stomach
1. A, C, and D
2. A
3. A
4. C
References
Kim KW, Choi BI, Han JK, et al: Postoperative anatomic and pathologic findings at CT following gastrectomy. Radiographics. 2002;22(2):323–336.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 86.
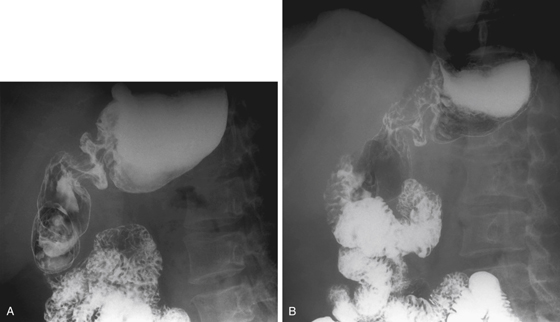
Comment
This case emphasizes the importance of having a correct and relevant patient history before doing a procedure. In this case, the history was not given with the imaging request, and the radiologist failed to obtain the history of prior gastric surgery from the patient. The stricture of the distal stomach was misdiagnosed as a possible malignancy (see figures). The stricture is actually a pseudotumor of the stomach caused by the large deformity that results from anastomosing a large lumen. This case is a reminder to residents in training that they are physicians and that no procedure should ever be undertaken without first talking to the patient (if possible) and obtaining a short, concise, and relevant history.
Pseudotumor of the stomach should not be confused with pseudolymphoma of the stomach, the appearance of which mimics an aggressive lymphoma or adenocarcinoma. Pseudolymphomas of the stomach are rare but should be included (near the bottom of the list) in the differential diagnosis of any large, seemingly aggressive lesion of the stomach.






