[level-membership-for-gastroenterology-and-hepatology-category]CASE 140
History: A 54-year-old man presents with rectal bleeding.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the most common site of colonic villous adenomas?
3. Which of the following statements regarding colonic polyps is true?
A. Of colonic polyps, 10% are adenomas.
B. Of colonic polyps, 10% are of flat morphology.
C. Of colonic polyps, 10% are found in the rectum.
D. Of colonic adenomas 1 to 2 cm in diameter, 10% contain carcinoma.
4. Which of these signs on barium enema describes a pedunculated polyp?
ANSWERS
CASE 140
Rectal Villous Adenoma
1. A, C, and E
2. C
3. D
4. C
References
O’Brien MJ, Winawer SJ, Zauber AG, et al: The National Polyp Study. Patient and polyp characteristics associated with high-grade dysplasia in colorectal adenomas. Gastroenterology. 1990;98(2):371–379.
Rubesin SE, Saul SH, Laufer I, et al: Carpet lesions of the colon. Radiographics. 1985;5:537–552.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 268.
Comment
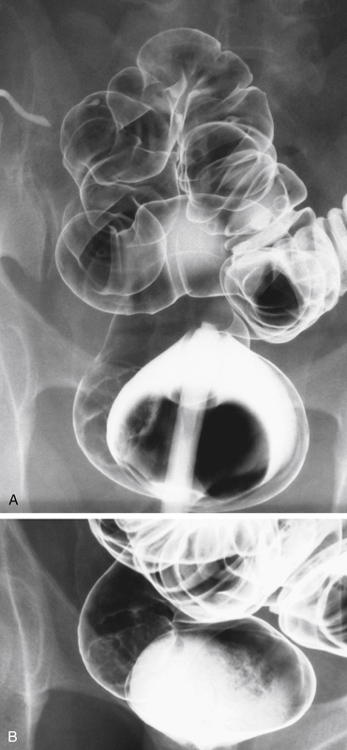
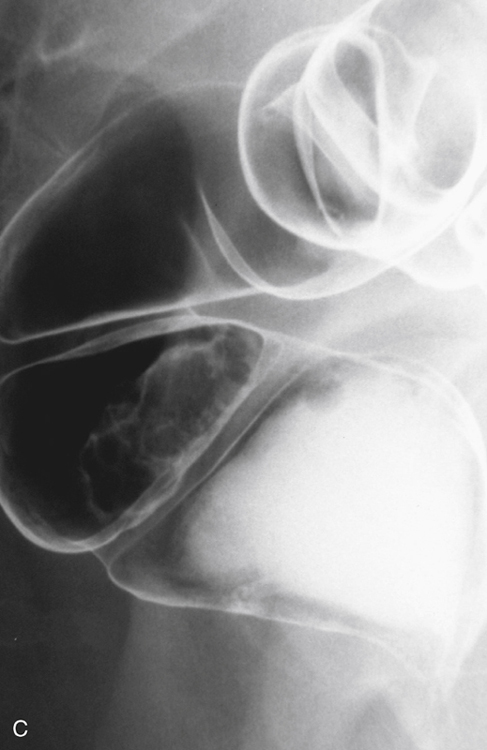
Neoplastic lesions of the colon usually manifest as polypoid protuberances into the lumen of the bowel. They occasionally grow superficially or even infiltrate through the wall of the bowel. The “carpet” lesion of the colon results when a neoplastic growth develops superficially along the mucosa rather than growing in a polypoid fashion. This growth produces a subtle irregularity of the mucosal surface, and the barium that becomes entrapped within the interstices of the lesion has the appearance of shag carpet—hence the terminology.
This subtle lesion is on the lateral rectal wall, is flat (instead of having the usual concavity), and is slightly irregular (see figures). Tumors that develop in this fashion typically occur in areas of the colon where the diameter is quite large. Most are found in the rectum and cecum and to a lesser extent in the ascending colon. These areas are where peristaltic activity is least likely to push an intraluminal lesion distally, which may promote intraluminal growth as seen in other areas.
Pathologically, these tumors tend to be predominantly villous adenomas and are potentially dangerous because many contain foci of malignancy. Some investigators consider villous adenoma as a premalignant lesion. It would be unusual for these lesions to be simple adenomas. The lesions typically are larger than 3 cm because they are often difficult to diagnose when they are small. Lacking the intraluminal component, the subtle mucosal irregularity can be appreciated only with good double-contrast technique. The incidence of carcinoma in colonic adenomas increases with increasing size and with villous histologic findings. Some large carpet lesions may have villous histologic features but turn out not to be malignant.
These lesions are usually too large to be removed endoscopically. Because of their lack of intraluminal components, they are not amendable to endoscopic removal.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 140
History: A 54-year-old man presents with rectal bleeding.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the most common site of colonic villous adenomas?
3. Which of the following statements regarding colonic polyps is true?
A. Of colonic polyps, 10% are adenomas.
B. Of colonic polyps, 10% are of flat morphology.
C. Of colonic polyps, 10% are found in the rectum.
[/not-level-membership-for-gastroenterology-and-hepatology-category]
