CHAPTER 14 Local Anesthetics
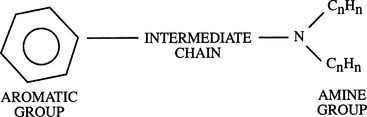
2 How are local anesthetics classified?


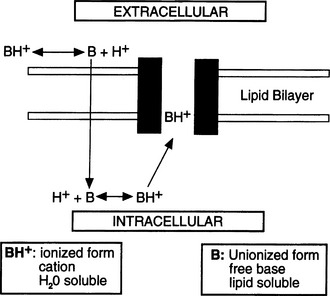
5 What is the mechanism of action of local anesthetics?
The cascade of events (Figure 14-2) follows:



6 Your patient states that he was told he is allergic to Novocain, which he received for a tooth extraction. Should you avoid using local anesthetics in this patient?
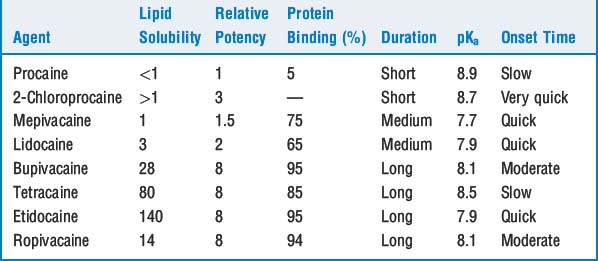
7 What determines local anesthetic potency?
The higher the solubility, the greater the potency (Table 14-1). This relationship is more clearly seen in isolated nerve than in clinical situations when factors such as vasodilation and tissue redistribution response to various local anesthetics influence the duration of local anesthetic effect. For example, high lipid solubility of etidocaine results in profound nerve blockade in isolated nerve. Yet, in clinical epidural use etidocaine is considerably sequestered in epidural fat, leaving a reduced amount of etidocaine available for neural blockade.
12 Which regional anesthetic blocks are associated with the greatest degree of systemic vascular absorption of local anesthetic?
13 Why are epinephrine and phenylephrine often added to local anesthetics? What cautions are advisable regarding the use of these drugs?
These drugs cause local tissue vasoconstriction, limiting uptake of the local anesthetic into the vasculature and thus prolonging its effects and reducing its toxic potential (see Question 14). Epinephrine, usually in 1:200,000 concentration, is also a useful marker of inadvertent intravascular injection. Epinephrine is contraindicated for digital blocks or other areas with poor collateral circulation. Systemic absorption of epinephrine may also cause hypertension and cardiac dysrhythmias, and caution is advised in patients with ischemic heart disease, hypertension, preeclampsia, and other conditions in which such responses may be undesirable.
14 How does a patient become toxic from local anesthetics? What are the clinical manifestations of local anesthetic toxicity?









15 Is the risk of cardiotoxicity the same with various local anesthetics?
 The ratio of the dosage required for irreversible cardiovascular collapse and the dosage that produces CNS toxicity is much lower for bupivacaine and etidocaine than for lidocaine.
The ratio of the dosage required for irreversible cardiovascular collapse and the dosage that produces CNS toxicity is much lower for bupivacaine and etidocaine than for lidocaine.

KEY POINTS: Local Anesthetics 
16 How will you prevent and treat systemic toxicity?




17 What is the risk of neurotoxicity with local anesthetics?
 Transient neurologic symptoms manifest in the form of moderate-to-severe pain in the lower back, buttocks, and posterior thighs. These symptoms appear within 24 hours of spinal anesthesia and generally resolve within 7 days. The delayed onset may reflect an inflammatory etiology for these symptoms. They are seen most commonly with lidocaine spinal anesthesia and are rare with bupivacaine. Patients having surgery in the lithotomy position appear to be at increased risk of neurologic symptoms following either spinal or epidural anesthesia.
Transient neurologic symptoms manifest in the form of moderate-to-severe pain in the lower back, buttocks, and posterior thighs. These symptoms appear within 24 hours of spinal anesthesia and generally resolve within 7 days. The delayed onset may reflect an inflammatory etiology for these symptoms. They are seen most commonly with lidocaine spinal anesthesia and are rare with bupivacaine. Patients having surgery in the lithotomy position appear to be at increased risk of neurologic symptoms following either spinal or epidural anesthesia.








1. Mulroy M.E. Systemic toxicity and cardiotoxicity from local anesthetics: incidence and preventive measures. Reg Anesth Pain Med. 2002;27:556-561.
2. Rosenblatt M.A., Abel M. Successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine-related cardiac arrest. Anesthesiology. 2006;105:217-218.
3. Strichartz G.R., Berde C.B. Local anesthetics. In: Miller R.D., editor. Anesthesia. ed 6. Philadelphia: Churchill Livingstone; 2005:573-603.
