CASE 139

History: A 42-year-old woman presents with a 2-week history of vomiting and diarrhea.
1. What should be included in the differential diagnosis of the imaging finding shown in the figure? (Choose all that apply.)
2. What is the most common cause of small bowel obstruction in young adults?
3. What finding is most consistently recognized in cross-sectional imaging of active Crohn’s disease?
4. Which of the following statements regarding Crohn’s disease is true?
B. The incidence among blacks and Native Americans is higher than in whites in North America.
C. A person with Crohn’s disease is more likely to have a relative with IBD.
D. The highest prevalence is among individuals 50 to 80 years old.
ANSWERS
CASE 139
Crohn’s Disease Small Bowel Obstruction
1. A, B, C, and E
2. A
3. D
4. C
References
Horsthuis K, Bipat S, Bennink RJ, et al: Inflammatory bowel disease diagnosed with US, MR, scintigraphy, and CT: meta-analysis of prospective studies. Radiology. 2008;247(1):64–79.
Wills JS, Lobis IF, Denstman FJ. Crohn disease: state of the art. Radiology. 1997;202(3):597–610.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 114
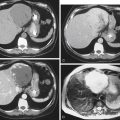
Comment
It is unusual for Crohn’s disease to manifest as a small bowel obstruction. However, a small percentage of patients present with small bowel obstruction, which often creates some diagnostic confusion. Why this obstruction occurs is unclear. It is probably a true inflammatory stricture further complicated by additional inflammation and edema, possibly around the site of a developing sinus or fistulous tract. CT, especially multidetector CT multiplanar imaging, has greatly increased the diagnostic capability of the physician (see figure). Although uncommon, a young patient presenting with small bowel obstruction and no history of prior abdominal surgery should raise the possibility of Crohn’s disease or acute appendicitis. Patients with Crohn’s disease presenting with acute small bowel obstruction represent about 2% of all newly seen disease. Acute small bowel obstruction is one of the few reasons that the treatment of these patients may be surgical. In some patients, nasogastric suction and high-dose steroids may relieve obstructive symptoms.