[level-membership-for-gastroenterology-and-hepatology-category]CASE 134
History: A 58-year-old woman presents with pruritus, rash, dyspepsia, and diarrhea.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the most common site of involvement with mastocytosis?
3. Which of the following conditions produces the greatest elevation of serum gastrin levels?
4. What is the most common abnormal finding in barium studies of the GI tract affected by mastocytosis?
C. Ileal mucosal fold thickening
ANSWERS
CASE 134
Mastocytosis of the Small Bowel
1. B, C, D, and E
2. A
3. A
4. B
References
Avila NA, Ling A, Worobec AS, et al: Systemic mastocytosis: CT and US features of abdominal manifestations. Radiology. 1997;202(2):367–372.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 127.
Comment
Numerous clinical conditions produce elevated serum gastrin levels. The best-known cause is Zollinger-Ellison syndrome, which results from a gastrin-producing tumor. Another condition associated with elevated gastrin is mastocytosis. Mastocytosis is an accumulation of mast cells in the skin and various other organs. Mast cells are responsible for storage and release of histamine. Histamine increases gastrin levels, although not to the extent seen in patients with Zollinger-Ellison syndrome (often >1000 pg/mL).
Mastocytosis typically involves the skin. When the mast cells are disturbed and release histamine, they produce yellow, red, or brown macules or papules, accounting for the disease description urticaria pigmentosa. It is less commonly known that other organs may be involved with a mast cell infiltrate; this occurrence is termed systemic mastocytosis. The GI tract (small bowel) is the second most commonly involved organ after the skin; the bone, liver, and spleen also can be involved. There can be both local and systemic release of histamine. Clinically, patients complain of bouts of diarrhea caused by malabsorption, flushing, and tachycardia. Alcohol consumption may precipitate the symptoms, and the condition is treated with histamine receptor antagonists.
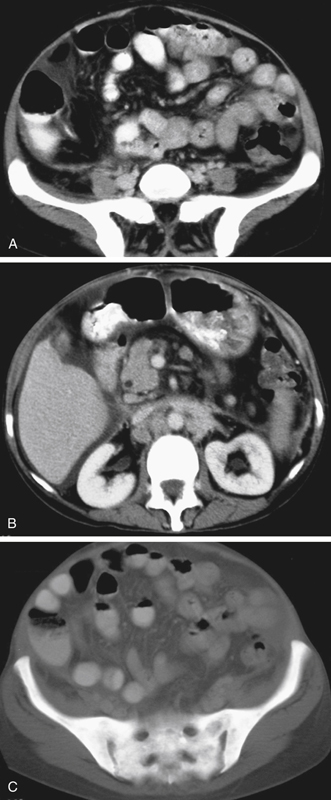
Radiologically, small bowel examination shows thickened folds and sometimes bowel wall thickening (see figures). Because of increased gastrin levels, there is a higher incidence of peptic ulcer disease and increased secretions in the small bowel. All these abnormalities may be present in a patient with Zollinger-Ellison syndrome. Other findings in patients with systemic mastocytosis include hepatosplenomegaly and lymphadenopathy (see figures). Mastocytosis can involve the bone marrow, producing diffuse sclerotic changes (see figures). In this case, all the visualized bones are quite dense.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 134
History: A 58-year-old woman presents with pruritus, rash, dyspepsia, and diarrhea.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the most common site of involvement with mastocytosis?
3. Which of the following conditions produces the greatest elevation of serum gastrin levels?
[/not-level-membership-for-gastroenterology-and-hepatology-category]
