CASE 132
1. What should be included in the differential diagnosis? (Choose all that apply.)
D. Mitral annular calcification
2. Which of the following diseases is not associated with mitral valve prolapse?
A. Syphilis
3. What is the most common cause of chordae tendineae rupture in this clinical setting?
D. Iatrogenic
4. What is the most appropriate next step in imaging?
B. CT
C. MRI
D. Angiography
ANSWERS
References
Bonow RO, Cheitlin MD, Crawford MH, et al. Task Force 3: valvular heart disease. J Am Coll Cardiol. 2005;45:1334–1340.
Enriquez-Sarano M, Akins CW, Vahanian A. Mitral regurgitation. Lancet. 2009;373(9672):1382–1394.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 192–193.
Comment
Pathology and Etiology
Mitral valve prolapse can involve all components of the mitral apparatus. Mitral valve prolapse has a 5% incidence in the general population. In Marfan syndrome, congenital prolapse occurs in the mitral and tricuspid valves because the valve leaflets are redundant. If prolapse is mild, the heart may be normal. More severe prolapse may result in severe regurgitation, subacute bacterial endocarditis, chest pain, or rarely death. Geometric distortion of the left ventricle can cause moderate mitral valve prolapse.
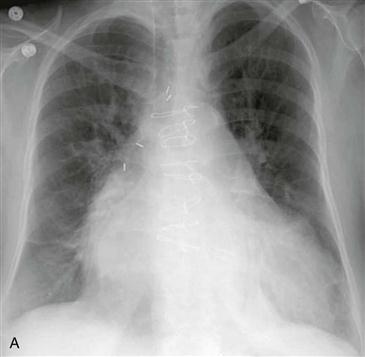
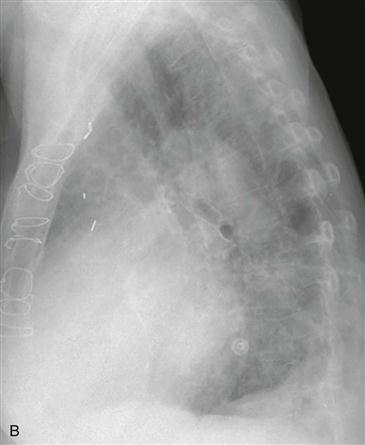
Imaging Findings
Findings of mitral valve prolapse on chest radiograph are similar to findings of mitral regurgitation from other causes: enlargement of the left atrium and ventricle (Figs. A and B). Mitral valve prolapse can be identified on echocardiography, and echocardiography can be used to grade the severity of prolapse and the presence and degree of regurgitation. Although angiography is not commonly performed for diagnosis, the angiographic hallmark of mitral valve prolapse is the passage of the leaflets behind the plane of the anulus into the left atrium.






