CASE 130
History: A 68-year-old man presents with anorexia, weight loss, and vomiting.
1. What should be included in the differential diagnosis of the imaging finding shown in the figure? (Choose all that apply.)
D. Transpyloric spread of lymphoma
E. Transpyloric spread of gastric cancer
2. What is the most common gastric malignancy?
3. This was a case of a malignancy crossing the pylorus. What is the most likely malignancy to cross the pylorus?
4. What is the most common gross morphology of gastric adenocarcinoma?
ANSWERS
CASE 130
Gastric Carcinoma Crossing the Pylorus
1. A, B, D, and E
2. A
3. A
4. B
References
Iyer R, Dubrow R. Imaging upper gastrointestinal malignancy. Semin Roentgenol. 2006;41(2):105–112.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 68.
Comment
About 90% to 95% of gastric malignancies are adenocarcinomas; about 4% are lymphomas; and the rest are a rare assortment of other lesions, mostly malignant gastrointestinal stromal tumors. It has long been taught that adenocarcinomas crossing the pylorus are very rare. Residents are taught that lymphomas have a greater disposition to cross the pylorus and affect the duodenum, with adenocarcinomas doing this much less often. Although this teaching is true, when the question which lesions are found to have crossed the pylorus in more cases is posed, the answer is found by simple logic. Although lymphomas have a greater tendency to cross the pylorus, they constitute only a tiny fraction of gastric malignancies compared with adenocarcinomas. The specific answer to a question phrased in such a manner is adenocarcinoma.
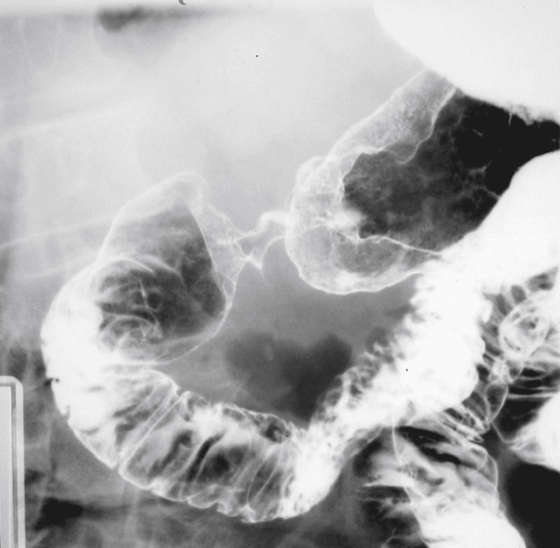
The idea that adenocarcinomas only rarely cross into the duodenum comes from early radiologic literature. Residents were taught that the pylorus was a “barrier” to the extension of the gastric lesion in that direction. However, more recent observations with microscopic support have suggested that transpyloric extension of gastric carcinomas may be more common than we believed. Studies have found that transpyloric extension may be 20%. This case demonstrates the point (see figure). Lesions in the prepyloric gastric antrum can result in two significant complications. Gastric outlet obstruction (often in a patient with no past history of peptic ulcer disease) is more common, but we must consider the possibility of transpyloric extension, even when not macroscopically visible.






