CHAPTER 13 Muscle Relaxants and Monitoring of Relaxant Activity
1 Describe the anatomy of the neuromuscular junction
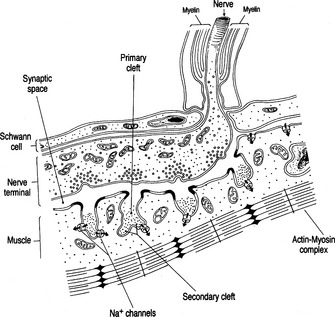
A motor nerve branches near its terminus to contact many muscle cells, losing myelin to branch further and come into closer contact with the junctional area of the muscle surface. Within the most distal aspect of the motor neuron, vesicles containing the neurotransmitter acetylcholine (ACh) can be found. The terminal neuron and muscle surface are loosely approximated with protein filaments, and this intervening space is known as the junctional cleft. Also contained within the cleft is extracellular fluid and acetylcholinesterase, the enzyme responsible for metabolizing ACh. The postjunctional motor membrane is highly specialized and invaginated, and the shoulders of these folds are rich in ACh receptors (Figure 13-1).
3 With regard to neuromuscular transmission, list all locations for acetylcholine receptors










6 How are muscle relaxants classified?
 Depolarizing relaxants: Succinylcholine (SCH) is two molecules of ACh bound together, an agonist at the NMJ, and the only depolarizing relaxant available clinically. As such, SCH binds to the α-subunits of the ACh receptor. After binding, SCH can open the ion channel and depolarize the end plate. Although SCH, like ACh, binds only briefly to the receptor, it is not hydrolyzed in the synaptic cleft by acetylcholinesterase. In fact, SCH molecules may unbind and rebind receptors repeatedly. SCH must diffuse away and be broken down in the plasma by enzymes called plasma- or pseudocholinesterase, and time for clearance from the body is an accurate measure of its duration of effect.
Depolarizing relaxants: Succinylcholine (SCH) is two molecules of ACh bound together, an agonist at the NMJ, and the only depolarizing relaxant available clinically. As such, SCH binds to the α-subunits of the ACh receptor. After binding, SCH can open the ion channel and depolarize the end plate. Although SCH, like ACh, binds only briefly to the receptor, it is not hydrolyzed in the synaptic cleft by acetylcholinesterase. In fact, SCH molecules may unbind and rebind receptors repeatedly. SCH must diffuse away and be broken down in the plasma by enzymes called plasma- or pseudocholinesterase, and time for clearance from the body is an accurate measure of its duration of effect.
8 If succinylcholine works so rapidly and predictably, why not use it all the time?







11 Review the properties of nondepolarizing muscle relaxants
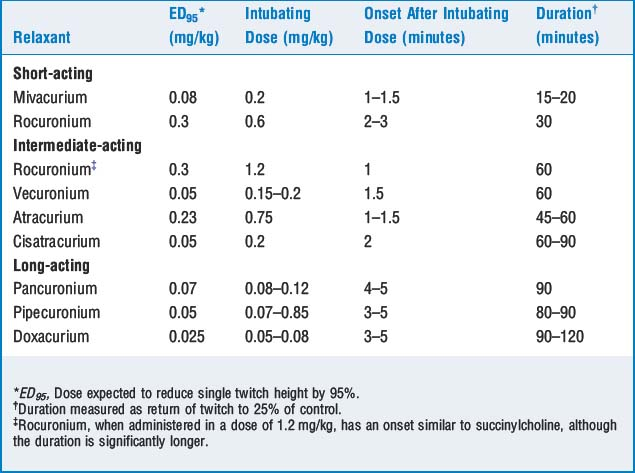
Nondepolarizing relaxants are competitive antagonists at the NMJ and are classified by their duration of action (short-, intermediate-, and long-acting). The doses, onset, and duration of effect are described in Table 13-1.
12 Review the metabolism of nondepolarizing neuromuscular blockers
 Aminosteroid relaxants (e.g., pancuronium, vecuronium, pipecuronium, and rocuronium) are diacetylated in the liver, and their action may be prolonged in the presence of hepatic dysfunction. Vecuronium and rocuronium also have significant biliary excretion, and their action may be prolonged with extrahepatic biliary obstruction.
Aminosteroid relaxants (e.g., pancuronium, vecuronium, pipecuronium, and rocuronium) are diacetylated in the liver, and their action may be prolonged in the presence of hepatic dysfunction. Vecuronium and rocuronium also have significant biliary excretion, and their action may be prolonged with extrahepatic biliary obstruction.


14 Review medications that potentiate the actions of muscle relaxants












19 Which mode is most commonly used to assess degree of blockade? How is it done?
KEY POINTS: Muscle Relaxants 
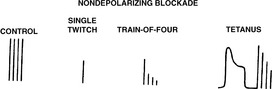
25 What are the characteristic responses to the various patterns of stimulation produced by nondepolarizing agents?


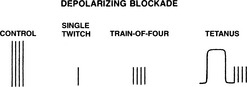
26 Summarize the characteristic responses to the various patterns of stimulation produced by depolarizing relaxants (succinylcholine)
The single-twitch, TOF, and tetanus amplitudes are uniformly decreased at any level of blockade. There is lack of fade in response to TOF and tetanus and lack of posttetanic facilitation. A desensitization or phase II blockade may develop with prolonged exposure to SCH. Phase II blockade has the same twitch characteristics as nondepolarizing blockade (Figure 13-3).
35 Review the clinical signs associated with return of adequate strength
| Test | Results | Percentage of Receptors Occupied |
|---|---|---|
| Tidal volume | >5 ml/kg | 80 |
| Single twitch | Return to baseline | 75–80 |
| Train of four | No fade | 70–75 |
| Sustained tetanus (50 Hz, 5 seconds) | No fade | 70 |
| Vital capacity | >20 ml/kg | 70 |
| Double-burst stimulation | No fade | 60–70 |
| Sustained tetanus (100 Hz, 5 seconds) | No fade | 50 |
| Inspiratory force | >−40 cm H2O | 50 |
| Head lift | Sustained 5 seconds | 50 |
| Hand grip | Return to baseline | 50 |
| Sustained bite | Sustained clenching of a tongue depressor | 50 |
36 A patient appears weak after pharmacologic reversal of neuromuscular blockade. What factors should be considered?







1. Herrerling T.M., Le N. Brief review: Neuromuscular monitoring: an update for clinician. Can J Anesth. 2007;54:58-72.
2. Hirsch N.P. Neuromuscular junction in health and disease. Br J Anaesth. 2007;99:132-138.
3. Martyn J.A.J., Richtsfeld M. Succinylcholine-induced hyperkalemia in acquired pathologic states. Anesthesiology. 2006;104:158-169.
4. Naguib M. Sugammadex: Another milestone in clinical neuromuscular pharmacology. Anesth Analg. 2007;104:575-581.
