[level-membership-for-surgery-category]
Procedure 13 In Situ Cubital Tunnel Decompression
 See Video 11: In Situ Cubital Tunnel Decompression
See Video 11: In Situ Cubital Tunnel Decompression
Indications
 In situ decompression of the ulnar nerve is indicated for patients with symptoms that are mild or intermittent (Table 13-1). If there is subluxation or instability of the ulnar nerve and/or ulnar nerve palsy owing to an abnormal osseous architecture of the elbow, in situ decompression is not indicated. In these situations, an anterior transposition is more appropriate to correct the anatomic problem.
In situ decompression of the ulnar nerve is indicated for patients with symptoms that are mild or intermittent (Table 13-1). If there is subluxation or instability of the ulnar nerve and/or ulnar nerve palsy owing to an abnormal osseous architecture of the elbow, in situ decompression is not indicated. In these situations, an anterior transposition is more appropriate to correct the anatomic problem.

Examination/Imaging
Clinical Examination








Surgical Anatomy
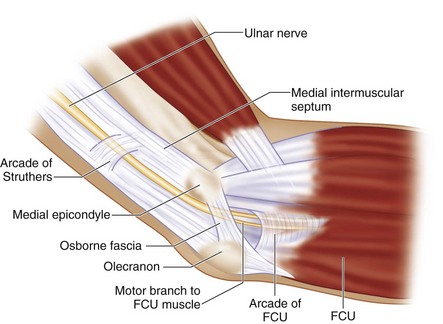
 The ulnar nerve is the terminal branch of the medial cord of the brachial plexus. Initially, the ulnar nerve lies medial to the axillary artery. In the upper arm, the ulnar nerve lies posteromedial to the brachial artery, posterior to the intermuscular septum, and anterior to the medial head of the triceps muscle. Approximately 8 cm proximal to the medial epicondyle is the arcade of Struthers, a thin fibrous band. At the elbow, the ulnar nerve travels posterior to the medial epicondyle and medial to the olecranon at the subcutaneous level, then it enters the cubital tunnel. The cubital tunnel is covered by fibroaponeurotic bands and the Osborne fascia (a ligament over the epicondylar groove), which is the fibroaponeurotic tissue between the two heads of the FCU. After passing through the cubital tunnel, the ulnar nerve travels deep into the forearm between the humeral and ulnar heads of the FCU. Distally, the ulnar nerve follows through the FCU to the deep flexor-pronator aponeurosis (Fig. 13-1).
The ulnar nerve is the terminal branch of the medial cord of the brachial plexus. Initially, the ulnar nerve lies medial to the axillary artery. In the upper arm, the ulnar nerve lies posteromedial to the brachial artery, posterior to the intermuscular septum, and anterior to the medial head of the triceps muscle. Approximately 8 cm proximal to the medial epicondyle is the arcade of Struthers, a thin fibrous band. At the elbow, the ulnar nerve travels posterior to the medial epicondyle and medial to the olecranon at the subcutaneous level, then it enters the cubital tunnel. The cubital tunnel is covered by fibroaponeurotic bands and the Osborne fascia (a ligament over the epicondylar groove), which is the fibroaponeurotic tissue between the two heads of the FCU. After passing through the cubital tunnel, the ulnar nerve travels deep into the forearm between the humeral and ulnar heads of the FCU. Distally, the ulnar nerve follows through the FCU to the deep flexor-pronator aponeurosis (Fig. 13-1).
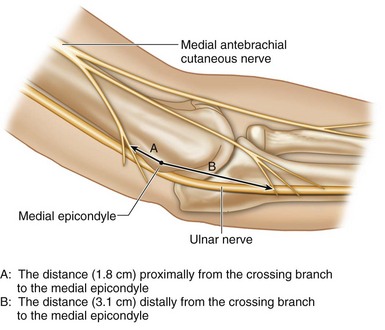
 The posterior branch of the medial antebrachial cutaneous nerve is at risk of injury during cubital tunnel surgery. The proximal crossing branch lies approximately 1.8 cm proximal to the medial epicondyle, whereas the distal crossing branch is about 3.1 cm distal to the medial epicondyle (Fig. 13-2).
The posterior branch of the medial antebrachial cutaneous nerve is at risk of injury during cubital tunnel surgery. The proximal crossing branch lies approximately 1.8 cm proximal to the medial epicondyle, whereas the distal crossing branch is about 3.1 cm distal to the medial epicondyle (Fig. 13-2).
 The ulnar nerve may be easily compressed at five sites (see Fig. 13-1).
The ulnar nerve may be easily compressed at five sites (see Fig. 13-1).
 The most common sites of ulnar nerve compression are the epicondylar groove and the cubital tunnel.
The most common sites of ulnar nerve compression are the epicondylar groove and the cubital tunnel.
Positioning
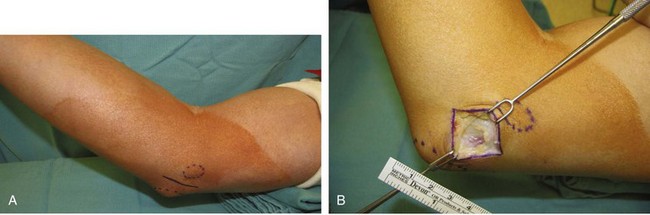
 The procedure is performed under tourniquet control. It can be done under regional or general anesthesia. The patient is positioned supine with the affected extremity on a hand table. The elbow is in 90-degree flexion, with some towels under the elbow to keep the elbow in flexion and supination posture. Placing these towels under the elbow will help in locating the medial epicondyle (Fig. 13-3).
The procedure is performed under tourniquet control. It can be done under regional or general anesthesia. The patient is positioned supine with the affected extremity on a hand table. The elbow is in 90-degree flexion, with some towels under the elbow to keep the elbow in flexion and supination posture. Placing these towels under the elbow will help in locating the medial epicondyle (Fig. 13-3).

Exposures

Procedure
Step 1


Step 2
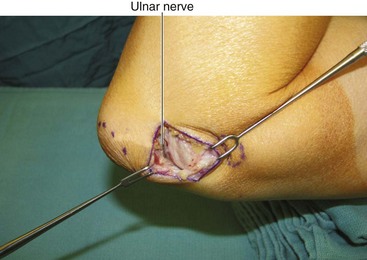
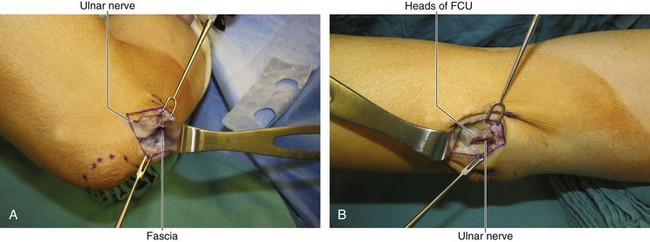
 After Osborne fascia release, the ulnar nerve is identified (Fig. 13-6).
After Osborne fascia release, the ulnar nerve is identified (Fig. 13-6).
 The skin is retracted proximally and distally at the medial epicondyle. The tightened fascia over the ulnar nerve can be checked using scissors; if the fascia is tight, it may be divided with scissors (Fig. 13-7A and B).
The skin is retracted proximally and distally at the medial epicondyle. The tightened fascia over the ulnar nerve can be checked using scissors; if the fascia is tight, it may be divided with scissors (Fig. 13-7A and B).
 Distally, the muscle bellies of the FCU should be released if ulnar nerve compression is discovered.
Distally, the muscle bellies of the FCU should be released if ulnar nerve compression is discovered.
Step 2 Pearls
The ulnar nerve is secured in its groove with areolar tissue and longitudinal feeding blood vessels. Freeing this areolar tissue will cause ulnar nerve subluxation. Only the compressive fascia band needs to be released, whereas the supporting soft tissue posterior to the ulnar nerve should not be disturbed.





Postoperative Care and Expected Outcomes


Miller RG, Hummel EE. The cubital tunnel syndrome: treatment with simple decompression. Ann Neurol. 1980;7:567-569.
Nathan PA, Istvan JA, Meadows KD. Intermediate and long-term outcomes following simple decompression of the ulnar nerve at the elbow. Chir Main. 2005;24:29-34.
Tanigughi Y, Takami M, Tamake T, et al. Simple decompression with small skin incision for cubital tunnel syndrome. J Hand Surg [Br]. 2002;27:559-562.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Procedure 13 In Situ Cubital Tunnel Decompression
See Video 11: In Situ Cubital Tunnel Decompression
Indications
In situ decompression of the ulnar nerve is indicated for patients with symptoms that are mild or intermittent (Table 13-1). If there is subluxation or instability of the ulnar nerve and/or ulnar nerve palsy owing to an abnormal osseous architecture of the elbow, in situ decompression is not indicated. In these situations, an anterior transposition is more appropriate to correct the anatomic problem.
Examination/Imaging
Clinical Examination
Surgical Anatomy
The ulnar nerve is the terminal branch of the medial cord of the brachial plexus. Initially, the ulnar nerve lies medial to the axillary artery. In the upper arm, the ulnar nerve lies posteromedial to the brachial artery, posterior to the intermuscular septum, and anterior to the medial head of the triceps muscle. Approximately 8 cm proximal to the medial epicondyle is the arcade of Struthers, a thin fibrous band. At the elbow, the ulnar nerve travels posterior to the medial epicondyle and medial to the olecranon at the subcutaneous level, then it enters the cubital tunnel. The cubital tunnel is covered by fibroaponeurotic bands and the Osborne fascia (a ligament over the epicondylar groove), which is the fibroaponeurotic tissue between the two heads of the FCU. After passing through the cubital tunnel, the ulnar nerve travels deep into the forearm between the humeral and ulnar heads of the FCU. Distally, the ulnar nerve follows through the FCU to the deep flexor-pronator aponeurosis (Fig. 13-1).
[/not-level-membership-for-surgery-category]
