CHAPTER 13
Biceps Tendon Rupture
Definition
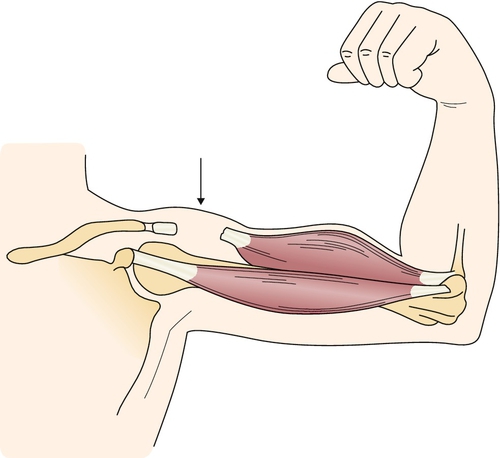
Biceps tendon rupture is either complete or partial disruption of the tendon of the biceps brachii muscle that can occur proximally or distally. The more common proximal ruptures are frequently seen in older individuals who have had chronic tendinosis of the long head of the biceps tendon associated with concomitant rotator cuff disease and degenerative joint disease of the shoulder [1] (Fig. 13.1). The incidence is 1.2 per 100,000 patients, with a majority on the dominant side of men who smoke and are in the fourth decade of life [2]. Most cases involve the long head of the biceps brachii and are manifested as a partial or complete avulsion from the superior rim of the anterior glenoid labrum [3]. Rupture of the proximal biceps tendon represents 90% to 97% of all biceps ruptures; it almost exclusively involves the long head [4] and is 7.5 times more likely in smokers [2].
Recent cadaveric study suggests that the relative avascularity of the long head of the biceps tendon may be a risk factor, as seen in many other tendon ruptures. Supplied through its osteotendinous and musculotendinous junctions and rarely branches from the anterior circumflex humeral artery traveling in a mesotenon, the long head of the biceps tendon has a hypovascular region in the border of two adjacent vascular territories. This region of limited arterial supply, 1.2 to 3 cm from the tendon origin, extends midway through the glenohumeral joint to the proximal intertubercular groove [5]. The distal biceps rupture is relatively uncommon and typically occurs in middle-aged men, although acute traumatic ruptures may occur in younger individuals or in anyone engaged in predisposing activities, such as forceful explosive contraction of the biceps. Patients with a distal biceps tendon rupture carry a risk of at least 8% for a rupture on the contralateral side [6]. This often develops suddenly with stressing of the flexor mechanism of the elbow. Distal biceps rupture usually occurs as a single traumatic event, such as with heavy lifting; it is often an avulsion of the tendon from the radial tuberosity, but it can also occur as a midsubstance tendon rupture [7].
Symptoms
Proximal ruptures are often asymptomatic and are commonly discovered with awareness of distal migration of the biceps brachii muscle mass, or they may occur suddenly by a seemingly trivial event. Often, individuals will note an acute “popping” sensation. The patient often takes one finger and points directly to the bicipital groove when describing the pain. Edema and ecchymosis may be seen with tendon rupture but also with other regional pathologic processes. The proximal ruptures are typically less painful but can be preceded by chronic shoulder discomfort [8]. An acute distal rupture is often associated with pain at the antecubital fossa that is typically aggravated by resisted elbow flexion. The pain is usually sharp initially but improves with time and is often described as a dull ache [9]. Swelling, distal ecchymosis, and proximal migration of the biceps brachii muscle mass accompany this injury with a magnitude dependent on the degree of injury. Younger, healthy patients may often present with a cosmetic rather than a functional complaint.
Physical Examination
Visual inspection of the biceps brachii, including comparison with the unaffected limb, is usually the first and most critical element in the physical examination of this condition. Advances in portability, training, and technology have led to a larger trend among physicians in various specialties to integrate diagnostic musculoskeletal ultrasound into the early phases of routine clinical assessment [10].
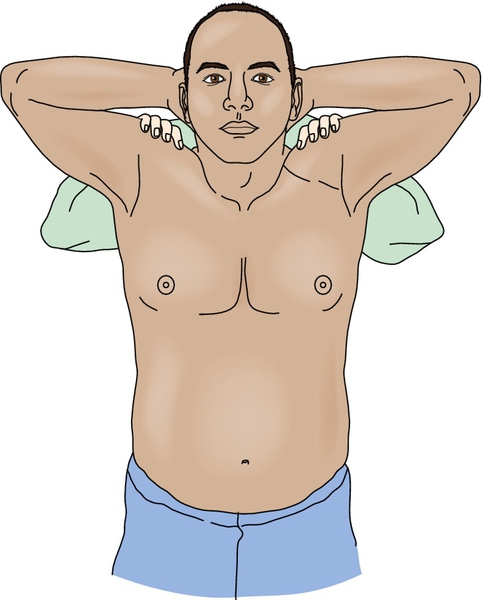
The Ludington test [11] is a recommended position in which to observe differences in the contour and shape of the biceps (Fig. 13.2). Diagnosis of complete ruptures is relatively easy; patients often come in aware of the biceps muscle retraction. Partial ruptures exist along a spectrum and can be more difficult to diagnose. The clinician should also assess for the presence of ecchymosis or swelling as a sign of acute injury. Palpation for point tenderness will often reveal pain at the rupture site. An effort should also be made to determine whether the rupture is complete by palpation and observation of the tendon. Thorough assessment of the shoulder and elbow should be made for range of motion and laxity. The Yergason [12] and Speed [13] tests (see Chapter 12), which are used in the assessment of bicipital tendinitis, are also recommended. Posterior dislocation of the long head of the biceps tendon has been reported [14] and may share some common physical examination findings but not muscle retraction.
In patients with inconsistent physical examination findings and questionable secondary gains, the American Shoulder and Elbow Surgeons subjective shoulder scale [15], a standardized scale of shoulder function with patient and physician components, has demonstrated acceptable psychometric performance for outcomes assessment in patients with shoulder instability, rotator cuff disease, and glenohumeral arthritis [16]. It is important to examine the entire shoulder and to keep in mind that it is a complex, inherently unstable, well-innervated joint that tends to function, and fail, as a unit; therefore, additional lesions that are the true pain generator may be evident. One study [17] looking at shoulder magnetic resonance findings showed no statistical relationship between the level of disability and either biceps tendon rupture or biceps tendinopathy; rather, disability was linked to supraspinatus tendon lesions and bursitis.
A thorough neurologic and vascular examination is performed, and findings should be normal in the absence of concomitant problems. Caution should be used with strength testing or end-range motion to avoid worsening of an incomplete tear.
Functional Limitations
The functional limitations are generally relatively minimal with proximal biceps rupture [18], and the patient’s concern is often centered around cosmetic considerations. More significant weakness of elbow flexion and supination is noted after a distal tendon disruption. Pain can be acutely limiting after both situations but is typically more of a problem in distal rupture. The primary role of the biceps brachii is supination of the forearm. Elbow flexion is functional by the action of the brachialis and brachioradialis. A degree of residual weakness with supination and elbow flexion, particularly after distal tendon rupture, can cause functional impairment for individuals who perform heavy physical labor [19]. Fatigue with repetitive work is also a common complaint with nonsurgically treated distal tendon ruptures [20]. The long head of the biceps is thought to play a role in anterior stability of the shoulder [21,22]; this is an issue for people who perform overhead activities (such as lifting, filing, and painting), powerlifting (in which the final 10% of strength is crucial), and nonsports activities in which the appearance of symmetry is important (such as modeling or bodybuilding).
Diagnostic Studies
The diagnosis of biceps brachii rupture is often made on a clinical basis alone. Magnetic resonance imaging is helpful in confirming the diagnosis and assessing the extent of the injury, but it should be performed in the FABS (flexed elbow, abducted shoulder, forearm supinated) position to obtain a true longitudinal view [23]; it is particularly useful in partial ruptures. Magnetic resonance imaging studies can also assess concomitant rotator cuff disease. Diagnostic ultrasound, which has grown in applicability and portability, may have a role in demonstrating not only proximal but also distal biceps tendon bifurcation [24]. Diagnostic ultrasound may be more cost-effective as an initial screening tool when no surgical injuries are suspected. Imaging of the entire insertion site as well as of elbow structures should be performed in distal ruptures [25]. Plain radiographs sometimes show hypertrophic bone formation related to chronic degenerative tendon abnormalities as a predisposition to rupture. Radiographs are also obtained in acute traumatic cases to rule out fractures and to identify developmental variants. Electrodiagnostic medicine consultation for possible peripheral nerve damage should be considered in cases with evidence of lower motor neuron findings or where the distribution of weakness is not fully accounted for by pain. Attention should be paid to median neuropathy at the elbow and, although it is technically difficult, to lateral antebrachial cutaneous nerve studies.
Treatment
Initial
For most patients, treatment of proximal biceps tears is conservative. Gentle range of motion exercises for prevention of contractures of the elbow and shoulder (adhesive capsulitis) can be started almost immediately. The function of the long head of the biceps tendon and its role in glenohumeral kinematics presently remain only partially understood because of the difficulty of cadaveric and in vivo biomechanical studies. Most treatment and rehabilitation efforts remain evidence based [26]. Surgery is rarely necessary because there is little loss of function with this tear, and the cosmetic deformity is generally acceptable without surgical repair. Young athletes or heavy laborers may be the exception; they typically need the lost strength that occurs with loss of the continuity of the biceps tendon [27]. Distal tears are more commonly referred to surgery acutely. However, initial treatment of partial distal ruptures consists of splint immobilization in flexion, which should be continued for 3 weeks. This is followed by a gradual return to normal activities. Analgesics, nonsteroidal anti-inflammatory drugs, topical agents (menthol-based or other custom compounded), therapeutic ultrasound, and ice may assist with the swelling and discomfort and facilitate rehabilitation efforts in both proximal and distal ruptures.
Rehabilitation
Nonsurgical treatment includes gentle range of motion exercises of the elbow and shoulder for contracture prevention. Modalities such as iontophoresis and therapeutic ultrasound can be used for pain control and prevention of contraction. Electrical stimulation is largely contraindicated in a partial tear (because of the concern of converting it to a complete tear) and not indicated in a complete tear. Gentle strengthening can typically be done after the acute phase in complete tears that are not going to be repaired because there is little chance of further injury. Partial ruptures can scar and remain in continuity [2].
Postoperative rehabilitation for distal biceps rupture repairs consists of immobilization of the elbow in 90 degrees of flexion for 7 to 10 days, followed by the use of a hinged flexion-assist splint with a 30-degree extension block for 8 weeks after surgery. Gentle range of motion and progressive resistance exercises are started initially; unlimited activity is not typically allowed until 5 months postoperatively [28].
Procedures
No procedures are performed in the direct treatment of biceps tendon rupture. Musculocutaneous nerve, upper trunk brachial plexus, and maybe even stellate ganglion blocks may have a role either perioperatively or palliatively in selected cases. Suprascapular nerve block or subacromial infiltration of local anesthetic may have a role in facilitation of rehabilitation therapies, including maintenance of range of motion and prevention of a secondary adhesive capsulitis. The author often coordinates such local anesthetic infiltrations just before physical or occupational therapy appointments. Caution should be exercised during passive stretching, and even then only by therapists who are familiar with suppression of protective mechanisms, to avoid further soft tissue damage at what may be atypical and asymmetric end-range motion. There may be a role for steroid injection in professional or elite athletes during critical phases of their season. In such cases, the subacromial approach is preferred with avoidance of direct needle entry into the biceps tendon. Pulsed radiofrequency of the suprascapular nerve may also have a longer term role in palliation of pain and has the advantage of not requiring steroid injection.
Surgery
Prompt assessment is necessary for complete distal biceps ruptures under consideration for surgical repair because muscle shortening will occur over time. The same is true for proximal ruptures in very active individuals who require maximal upper body strength for their vocation or sport. Optimal surgical outcomes are obtained if treatment occurs within the first 4 weeks after injury. Partial distal ruptures are generally observed nonoperatively until a complete rupture occurs. Several techniques, including the two-incision, buttonhole, and Boyd-Anderson approaches, are used. More recently, a sonographically guided, mini-open technique involving one incision giving access to three peripectoral anatomic zones has been described [29]. The goal of surgical treatment is to restore strength of supination and flexion. For distal repairs, this is typically performed by a two-incision technique involving reinsertion of the biceps tendon to the radial tuberosity [30]. A single-incision technique with use of suture anchors in the bicipital tuberosity has shown excellent long-term functional results by the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire [31].
Potential Disease Complications
Complications from isolated biceps rupture are relatively rare. Partial tears can become complete tears. Attention should be given to potential contracture formation. Median nerve compression has been reported presumably to be related to an enlarged synovial bursa associated with a partial distal biceps tendon rupture [32]. Isolated antebrachial cutaneous neuropathy, due to traction from the biceps tendon displacing the nerve laterally with alleviation of symptoms after proximal biceps tenodesis, has been reported [33]. Compartment syndrome has also been reported in proximal biceps rupture in a patient receiving systemic anticoagulation [34]. The risk-benefit ratio of discontinuing drugs known to have an association with tendon rupture should be ascertained.
Potential Treatment Complications
Analgesics and nonsteroidal anti-inflammatory drugs have well-known side effects that most commonly affect the gastric, hepatic, and renal systems. Advancement of the extent of the rupture can occur with overly aggressive strengthening measures and passive stretching. The potential for serious surgical complications is most significant with distal rupture because of the important neurovascular structures in that region, including the median and radial nerves and brachial artery and vein [26]. The complication rate increases with the length of time after rupture that surgery is performed. Proximal radial-ulnar synostosis and heterotopic ossification have also been reported as rare postsurgical complications [21], as has humeral fracture after subpectoral biceps tenodesis [35]. Stiffness and contractures are possible with or without surgical intervention.






