
History: A 57-year-old man presents with 4 days of nausea and vomiting, abdominal pain, and distention.
1. Which of the following should be included in the differential diagnosis for this abnormality (gastric distention)? (Choose all that apply.)
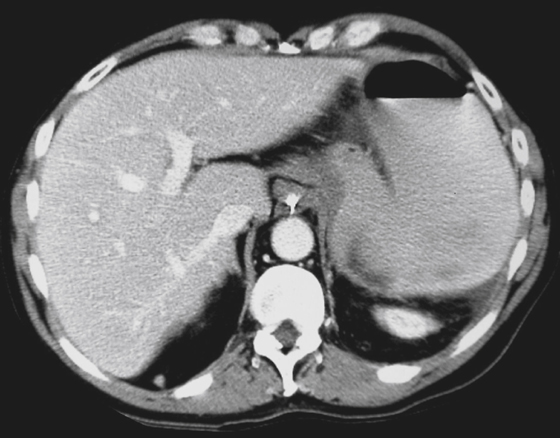
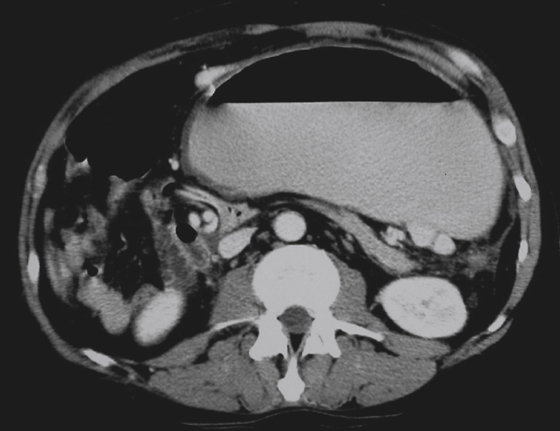
2. Review the provided images. What is the single best diagnosis?
A. Diaphragmatic incarcerated hernia
B. Organoaxial gastric volvulus
C. Mesenteroaxial gastric volvulus
D. Para-esophageal hiatal incarcerated hernia
3. What is the treatment for the condition demonstrated in the provided images?
D. Nothing, the condition is self-limiting and reversible
4. Which of the following statements about gastric volvulus is true?
A. Occurs more commonly in female patients.
ANSWERS
CASE 13
Gastric Volvulus
1. A, B, D, and E
2. C
3. C
4. D
Reference
Peterson CM, Anderson JS, Hara AK, et al: Volvulus of the gastrointestinal tract: appearances at multimodality imaging. Radiographics. 2009;29:1281–1298.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 54-55.
Comment
To understand gastric volvulus, it is useful to consider the anatomy of the stomach and its attachments. The stomach is fixed to the diaphragm just above the gastroesophageal junction proximally and to the retroperitoneum at the first duodenal flexure distally. In between, the stomach is attached posteriorly by a fan-shaped mesentery (the mesogastrum).
There are two varieties of gastric volvulus. The axis of the organ is the long axis of the stomach, an imaginary line drawn between the gastroesophageal junction and the cardia to the pylorus. Organoaxial volvulus refers to rotation of the stomach upward along this long axis. In this condition, the greater curvature is thrown up cephalad to the lesser curvature, a horizontal-lie stomach. This is the most common type; it is usually chronic and asymptomatic and seen in older patients. Strangulation and necrosis have been reported in 5% to 25% of patients with this type.
The axis of the mesentery is the middle of the mesenteric fan, the gastrohepatic omentum, a line passing through the middles of the lesser and greater curvatures. Mesenteroaxial volvulus refers to left-to-right or right-to-left rotation of the stomach about this axis. This brings the pylorus close to the cardia, and the antrum is thrown cephalad to the fundus (see figures). This type of volvulus is more serious and more likely to be incarcerated.
Mesenteroaxial volvulus can occur, albeit infrequently, with stomachs in the normal epigastric location. Variations of mesenteroaxial volvulus is more often seen when the stomach has migrated (usually owing to massive hiatal herniation) or where the stomach has been displaced by left diaphragm elevation. In these scenarios, the gastric mesentery has been considerably distorted and/or disrupted with the migration.
Some patients have few or no symptoms and have the condition a long time. However, when the torsion begins to obstruct or affect the vascular supply (see figures), the patient presents with symptoms ranging from nausea and vomiting to severe pain to cardiovascular collapse from gastric necrosis. Because of these potential risks, it is imperative that the referring service be made aware of an asymptomatic or minimally symptomatic gastric volvulus.






