[level-membership-for-gastroenterology-and-hepatology-category]CASE 127
History: A woman was involved in a high-speed motor vehicle accident.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the common perception error in right-sided rupture?
A. Mistaken for right basal contusion
B. Mistaken for right pleural effusion
C. Mistaken for right lower lobe collapse
D. Mistaken for elevation or eventration of the intact hemidiaphragm
3. Which of the following statements regarding blunt traumatic diaphragmatic injury is true?
A. Injury is usually a small linear tear.
B. Most are posterolateral and radial.
C. Injury usually involves the peripheral diaphragm.
D. Right diaphragm rupture is more common than left.
4. What other visceral injury occurs most commonly with left diaphragmatic injury?
ANSWERS
CASE 127
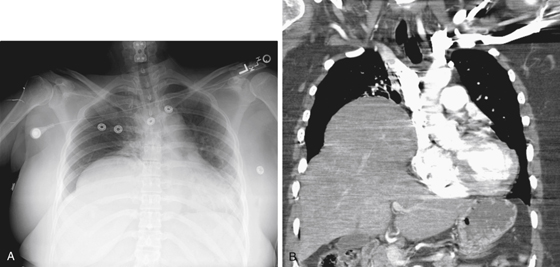
Diaphragmatic Rupture with the Liver in the Chest
1. A, B, C, and E
2. D
3. B
4. C
References
Eren S, Kantarci M, Okur A. Imaging of diaphragmatic rupture after trauma. Clin Radiol. 2006;61(6):467–477.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 326.
Comment
Most diaphragmatic ruptures are not as dramatic as the one shown in this case. This patient was involved in a high-speed motor collision. The supine portable image of the chest ought to arouse suspicion immediately because of what appears to be a high, rounded right-sided diaphragm (see figures). CT is the examination of choice (see figures), but it can miss small diaphragmatic tears. The likelihood of a diaphragmatic tear is eight times greater on the left side compared with the right side. It is believed that the liver absorbs some of the traumatic shock that would have been otherwise transmitted in its entirety to the diaphragm.
Although autopsy results put the incidence of diaphragmatic rupture at 5% to 6%, it is much lower clinically and radiologically. The reasons are that many of the patients die before reaching the hospital and the diagnosis is often difficult, even with CT. When discovered, a diaphragmatic tear should be surgically repaired. Most tears result in bowel in the lower chest, and the risk of future bowel obstruction, ischemia, or gastric volvulus is increased; this is generally applicable to right-sided tears as well. Almost every practicing radiologist has examined patients with bowel and in some cases liver in their chest who have no complaints relative to that finding. It is more than an “incidental” finding and should be handled as a significant finding. Other CT findings include discontinuation of the diaphragmatic stripe; this should be evaluated in cases of blunt severe abdominal trauma, especially so if a liver laceration is identified.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 127
History: A woman was involved in a high-speed motor vehicle accident.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the common perception error in right-sided rupture?
A. Mistaken for right basal contusion
B. Mistaken for right pleural effusion
C. Mistaken for right lower lobe collapse
D. Mistaken for elevation or eventration of the intact hemidiaphragm
3. Which of the following statements regarding blunt traumatic diaphragmatic injury is true?
A. Injury is usually a small linear tear.
B. Most are posterolateral and radial.
[/not-level-membership-for-gastroenterology-and-hepatology-category]
