CASE 126
History: A 26-year-old woman presents with a 1-year history of dyspepsia, nausea, vomiting, dark stools, and diarrhea.
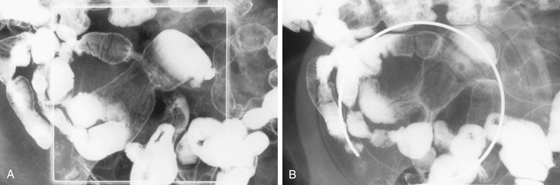
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. Which of the following statements about Meckel’s diverticula is true?
A. If a Meckel’s diverticulum is symptomatic, the most common manifestation is obstruction.
B. Meckel’s diverticula can contain ectopic pancreatic tissue.
C. Meckel’s diverticula are more common in women.
D. Of Meckel’s diverticula, 80% are asymptomatic.
3. Which of the following statements about the imaging findings of Meckel’s diverticula is false?
A. A Meckel’s diverticulum may appear on CT scan as an elongated ileal polyp.
B. Plain radiographs visualize about 50% of Meckel’s enteroliths.
C. A persistent vitelline artery on angiography is diagnostic.
D. An inverted diverticulum has a “picket fence” appearance on enteroclysis.
4. Which of the following statements about the scintigraphic diagnosis of Meckel’s diverticula is true?
A. The administered agent (99mTc pertechnetate) is specifically taken up by gastric mucosa only.
B. Of Meckel’s diverticula, 90% contain gastric mucosa allowing scintigraphic detection.
C. Pentagastrin and glucagon are useful.
D. Cimetidine increases tracer secretion.
ANSWERS
CASE 126
Meckel’s Diverticulum
1. A, B, D, and E
2. B
3. D
4. C
References
Elsayes KM, Menias CO, Harvin HJ, et al: Imaging manifestations of Meckel’s diverticulum. AJR Am J Roentgenol. 2007;189(1):81–88.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 142.
Comment
Meckel’s diverticulum is the most common congenital anomaly of the intestines; it occurs in 3% of the population. Meckel’s diverticulum represents incomplete obliteration of the omphalomesenteric duct (also called vitelline duct), which is an embryologic structure. Most Meckel’s diverticula do not cause symptoms. However, almost half of these diverticula contain gastric mucosa that may be functional and may produce pain, ulceration, and bleeding (see figures). Meckel’s diverticulum scan, in which 99mTc pertechnetate is used and is taken up by the gastric mucosa, can detect areas of ectopic gastric mucosa. However, this test is not always reliable. Other complications of Meckel’s diverticula include obstruction caused by either invagination and intussusceptions or formation of a large enterolith. Malignancy is rarely encountered.
Enteroliths are rare, forming in less than 10% of cases of symptomatic Meckel’s diverticula, and do not always calcify. When they do calcify, enteroliths may produce bleeding or obstruction. Major differential considerations include a gallstone that has eroded into the gastrointestinal tract, the so-called gallstone ileus syndrome, or a calcified appendicolith.






