CASE 125
History: No patient history is available.
1. Which of the following valves can be evaluated on the MRI four-chamber view? (Choose all that apply.)
A. Mitral
B. Tricuspid
C. Aortic
D. Pulmonic
2. What imaging planes are shown?
A. Vertical long-axis and four-chamber
B. Vertical long-axis and left ventricular outflow tract
C. Left ventricular outflow tract and four-chamber
D. Right ventricular outflow tract and short-axis
A. Mitral
B. Tricuspid
C. Pulmonic
D. Aortic
4. In addition to the abnormal valve, what is the other finding?
B. Cardiac mass
ANSWERS
Reference
Betrián Blasco P, Gallardo Agromayor E. Ebstein’s anomaly and left ventricular noncompaction association. Int J Cardiol. 2007;119(2):264–265.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, p 54.
Comment
Presentation and Associations
Ventricular noncompaction is a more recently described primary cardiomyopathy. Patients may be asymptomatic or may present with tachyarrhythmia, congestive heart failure, or cardiac thromboembolism. Pathologic noncompaction is occasionally associated with other cardiac conditions, including atrial septal defect, ventricular septal defect, pulmonic stenosis, partial anomalous pulmonary venous return, and Ebstein anomaly.
Imaging
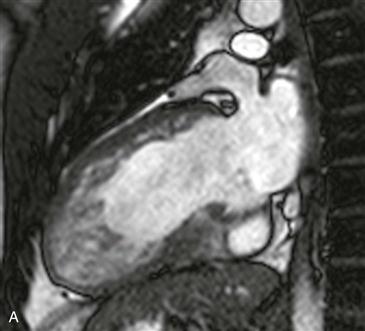
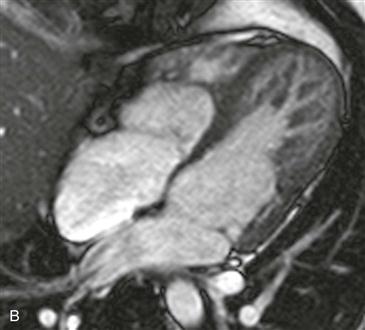
Cine steady-state free precession (SSFP) vertical long-axis and four-chamber images show prominent trabeculation with a distinct two-layered appearance of the left and right ventricular myocardium (Figs. A and B). There are deep intertrabecular recesses, and the measured ratio of noncompacted to compacted myocardium is elevated, measuring greater than 2.3 at end-diastole. This appearance fulfills the MRI diagnostic criterion for pathologic ventricular noncompaction. An additional observation is ventricular displacement of the tricuspid valve with respect to the mitral valve, consistent with Ebstein anomaly (Fig. B).






