CASE 124

History: A 54-year-old woman presents with right upper quadrant pain, jaundice, and fever.
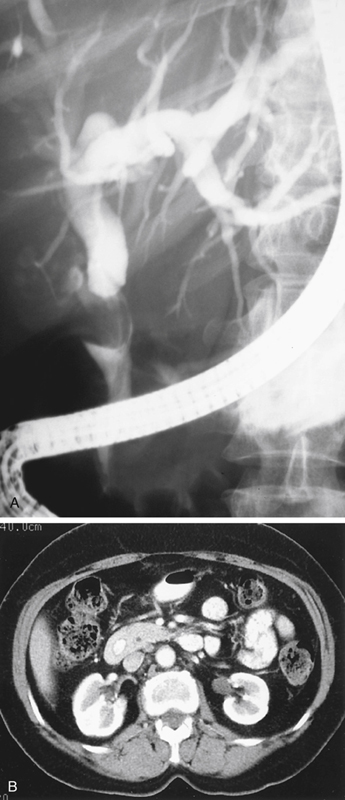
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the mechanism of Mirizzi’s syndrome?
A. A gallstone eroded into the common hepatic duct
B. A gallstone passed into the common bile duct
C. A gallstone impacted in the cystic duct
D. A gallstone eroded into the duodenum
3. What major iatrogenic complication is associated with this condition?
A. Surgical ligation of the common hepatic duct
B. Cholecystoduodenal fistula formation
C. Perforation of the gallbladder
4. What is the most common cause of obstructive jaundice?
ANSWERS
CASE 124
Mirizzi’s Syndrome
1. A, B, D, and E
2. C
3. A
4. B
References
Becker CD, Hassler H, Terrie F. Preoperative diagnosis of the Mirizzi syndrome: limitations of sonography and computed tomography. AJR Am J Roentgenol. 1984;143(3):591–596.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 231.
Comment
Mirizzi’s syndrome is an uncommon condition that occurs when a stone becomes impacted in the cystic duct or neck of the gallbladder. This type of impaction is very common, but in Mirizzi’s syndrome a severe local inflammatory response occurs. The affected area is critical because there are several ducts and crossing vessels in the region. The inflammatory response produces a mass or tumor effect in the area. The inflammatory mass impinges on the common hepatic and bile ducts, producing varying degrees of narrowing or obstruction. The intrahepatic bile ducts may become dilated proximal to the obstruction. Secondary involvement of the major vessels in the area can occur. There is also associated cholecystitis because the gallbladder is now obstructed.
The major concern for physicians encountering this condition is not the inflammation itself but the difficulty in making an appropriate diagnosis and performing corrective surgery. With the inflammatory mass effect and the bile duct dilation, the condition may mimic a neoplasm of either the gallbladder or the bile ducts (see figures). Adenopathy may have a similar appearance. These changes are most confusing on endoscopic retrograde cholangiopancreatography (ERCP).
Prompt surgical intervention is typically warranted. For the surgeon, the difficulty arises in identifying and isolating the correct ducts. Often the common hepatic duct is mistaken for the cystic duct, and ligation of the common hepatic duct ensues, producing disastrous complications. When possible, a stent can be placed in the extrahepatic ducts at ERCP to help identify them for the surgeon. The syndrome is named for Mirizzi, an Argentinian physician who described it in 1948.






