[level-membership-for-gastroenterology-and-hepatology-category]CASE 123
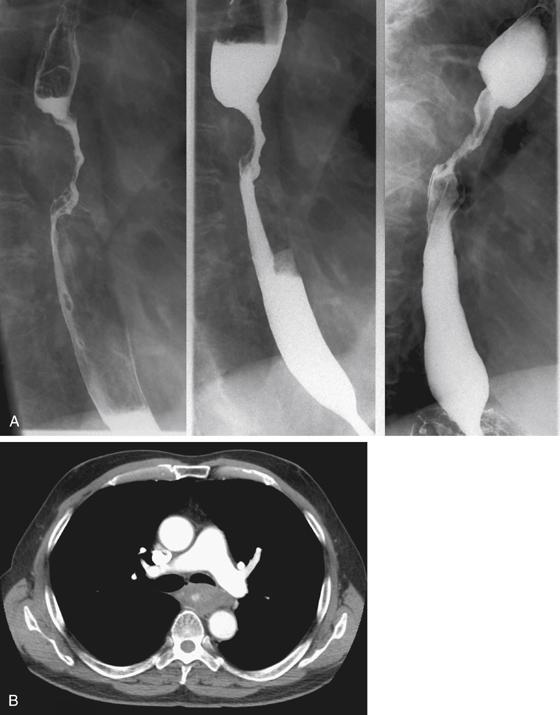
History: A 71-year-old man has a 16-month history of suprasternal dysphagia, which is worse with solids; the dysphagia has been worse in the last 8 months, now requiring food to be chewed to a puree consistency.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. Endoscopic biopsy confirms a malignant lesion. Which one of the following is most likely?
3. With a diagnosis of esophageal squamous cell carcinoma, what is the best choice of imaging modality to assist in therapeutic planning?
4. Which finding relevant to CT tumor staging is shown in figure 2?
ANSWERS
CASE 123
Esophageal Squamous Cell Carcinoma
1. A, B, C, and E
2. D
3. C
4. B
References
Iyer R, Dubrow R. Imaging upper gastrointestinal malignancy. Semin Roentgenol. 2006;41(2):105–112.
Levine MS. Esophageal cancer: radiologic diagnosis. Radiol Clin North Am. 1997;35(2):265–279.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 23.
Comment
Most esophageal cancers in Western countries are squamous cell carcinomas. Until the middle of the 20th century, squamous cell carcinomas accounted for more than 90% of esophageal malignancies. The other common tumor is adenocarcinoma, which has increased in frequency in recent decades so that the prevalence of the two primary esophageal tumors is now more equal.
The diagnosis of esophageal cancer is suggested on barium swallow by various appearances. Early esophageal cancer may appear as a superficial plaque or ulceration. Advanced disease is seen as a stricture, a mass, a circumferential infiltration, or an ulceration (see figures).
Prognosis for a patient with esophageal cancer is poor. Accurate staging is required for prognosis and therapeutic planning. Stage I disease is associated with 5-year survival rates of 60% to 70%; stage II disease, 40% to 50%; stage III disease, 15% to 25%; and stage IV disease, less than 10%. The TNM (tumor, node, metastasis) staging system is widely used. Accurate T classification is particularly important to determine tumor resectability. T4 tumors invading local structures are subclassified as T4a or T4b. T4a tumors, which have invaded structures such as pleura, pericardium, or diaphragm, are resectable. T4b tumors are unresectable, having invaded aorta, vertebral body, or trachea or bronchus (see figures).
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 123
History: A 71-year-old man has a 16-month history of suprasternal dysphagia, which is worse with solids; the dysphagia has been worse in the last 8 months, now requiring food to be chewed to a puree consistency.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. Endoscopic biopsy confirms a malignant lesion. Which one of the following is most likely?
3. With a diagnosis of esophageal squamous cell carcinoma, what is the best choice of imaging modality to assist in therapeutic planning?
[/not-level-membership-for-gastroenterology-and-hepatology-category]
