CASE 123
1. What should be included in the differential diagnosis for restrictive cardiomyopathy? (Choose all that apply.)
C. Amyloidosis
D. Doxorubicin (Adriamycin) therapy
E. Sarcoidosis
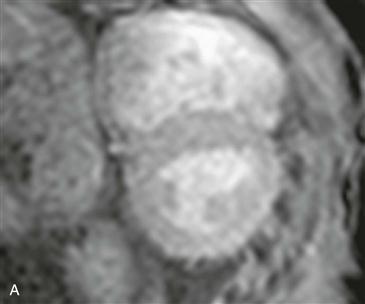
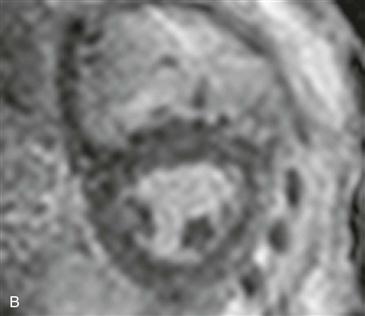
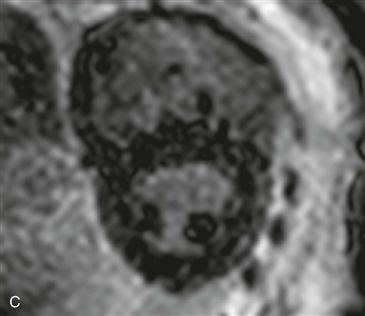
2. What imaging sequence is shown in Figs. A–C?
A. Steady-state free precession (SSFP)
B. Look locker (cine inversion recovery)
C. Black blood
3. What is abnormal about the images?
A. Nothing
B. Myocardium is nulled before blood pool.
D. Transmural late gadolinium enhancement in Fig. A
4. What additional finding on late gadolinium enhancement MRI would support the most likely diagnosis based on these figures?
A. Patchy enhancement not corresponding to an arterial distribution
B. Transmural enhancement in the territory of the left anterior descending (LAD) coronary artery
ANSWERS
References
Maceira AM, Joshi J, Prasad SK, et al. Cardiovascular magnetic resonance in cardiac amyloidosis. Circulation. 2005;111(2):186–193.
Ordovas KG, Higgins CB. Delayed contrast enhancement on MR images of myocardium: past, present, future. Radiology. 2011;261(2):358–374.
Vogelsberg H, Mahrholdt H, Deluigi CC, et al. Cardiovascular magnetic resonance in clinically suspected cardiac amyloidosis: noninvasive imaging compared to endomyocardial biopsy. J Am Coll Cardiol. 2008;51(10):1022–1030.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, p 286 (figure only).
Comment
Overview
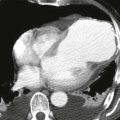
Cardiac amyloidosis is a common cause of secondary restrictive cardiomyopathy. Amyloid fibrillar proteins deposit in myocardium and lead to reduced ventricular compliance and diastolic function. Patients present with restrictive or constrictive physiology. Common symptoms include lower extremity edema, ascites, and dyspnea. MRI can differentiate constrictive pericarditis from restrictive cardiomyopathy. Constrictive pericarditis typically has pericardial thickening greater than or equal to 4 mm, whereas restrictive cardiomyopathy does not. Many causes of restrictive cardiomyopathy, such as amyloidosis, have characteristic appearances on late gadolinium enhancement imaging.
Evaluation
Abnormal myocardial nulling before blood pool nulling is likely secondary to cardiac deposition of amyloid protein. Amyloid deposition disrupts gadolinium kinetics and is responsible for loss of contrast between normal and abnormal myocardium when patients undergo late gadolinium enhancement imaging 8 minutes or longer after contrast agent injection. In patients with suspected cardiac amyloidosis, late gadolinium enhancement imaging ideally should be performed 5 to 8 minutes after contrast agent administration to maximize the difference between normal and abnormal myocardium. Diffuse subendocardial enhancement affecting the right and left ventricles is a characteristic enhancement pattern seen in cardiac amyloidosis. An additional finding includes wall thickening in affected myocardium.