CASE 122


1. What should be included in the differential diagnosis? (Choose all that apply.)
B. Vasculitis
C. Tumor
2. Which of the following conditions is likely associated with this lesion?
A. Stroke
3. Which of the following would be the most likely diagnosis if this patient also had bilateral heterogeneously enhancing adrenal masses?
A. Vasculitis
B. Tumor
4. Aortic intimal sarcoma most commonly occurs in what gender and age group?
A. Elderly men
D. Children
ANSWERS
References
Crone KG, Bhalla S, Pfeifer JD. Aortic intimal sarcoma detected on helical CT. J Thorac Imaging. 2004;19(2):120–122.
Kato W, Usui A, Oshima H, et al. Primary aortic intimal sarcoma. Gen Thorac Cardiovasc Surg. 2008;56(5):236–238.
Comment
Epidemiology and Treatment
Aortic intimal sarcoma is an exceptionally rare tumor of vascular origin. Most reported cases originate in the abdominal aorta. This tumor is often diagnosed late because both clinical presentation and imaging findings mimic atheromatous plaque. Symptoms are usually secondary to thromboembolic events with tumor embolism causing claudication, bowel ischemia, renal infarcts, or stroke. Prognosis is poor because the tumor tends to metastasize early. Treatment is surgical resection in patients without evidence of metastatic disease.
Imaging
This entity should be considered when an irregularly shaped lesion arises from the aortic wall. There is no evidence of dissection or penetrating ulcer. The most helpful imaging finding is the presence of an associated paraaortic mass that is contiguous with the intraluminal lesion. As in this case, the diagnosis is usually made at the time of surgery because the lesion is thought to represent an atheromatous plaque.
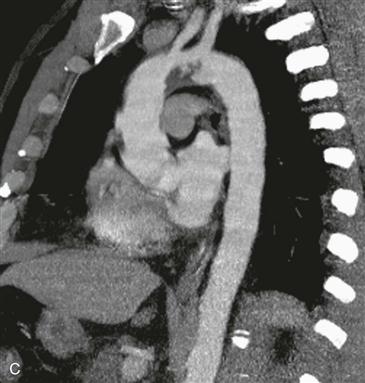
Coronal, axial, and oblique sagittal images (Figs. A–C) show an irregularly shaped mass arising from the inferior wall of the proximal aortic arch. The patient in this case presented with a frontal lobe infarct and a cold, ischemic left arm from tumor embolism into the left brachial artery. The preoperative diagnosis was a large atheroma in the aortic arch. Pathology showed the lesion was an intimal sarcoma.






