CASE 121
History: A 45-year-old woman presents with nausea and dyspepsia.
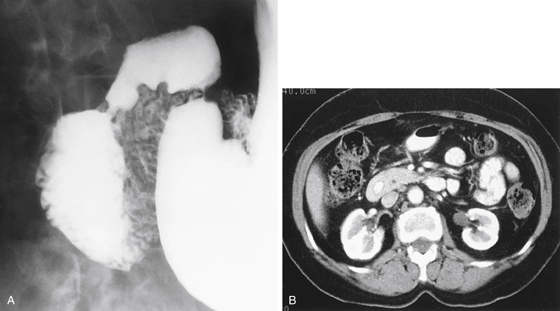
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
B. Superior mesenteric artery (SMA) syndrome
2. What is the most common presentation of annular pancreas?
3. Which of the following statements regarding imaging of annular pancreas is true?
A. A radiologically incomplete annulus will not result in obstruction.
B. Pancreas divisum is present in about 3% of patients with annular pancreas.
4. What portion of the embryologic pancreas becomes the uncinate process?
ANSWERS
CASE 121
Annular Pancreas
1. A, C, D, and E
2. D
3. D
4. D
References
Jayaraman MV, Mayo-Smith WM, Movson JS, et al: CT of the duodenum: an overlooked segment gets its due. Radiographics. 2001;21:S147–S160.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 152.
Comment
The embryologic development of the pancreas is complex and can lead to a variety of anomalies. Some are of no clinical significance, whereas others may present difficulties early or later in life. The pancreas forms as two distinct buds off the biliary or hepatic bud, which comes from the midgut. These buds are the ventral and dorsal pancreatic buds. The dorsal pancreatic bud is to the left of the midline and eventually forms the body and tail of the pancreas. The ventral bud develops to the right of the duodenum. It must rotate, along with the duodenum, to the left. After the ventral and dorsal buds fuse, this ventral bud becomes the head and uncinate process of the pancreas. Failure of fusion results in pancreatic divisum.
Annular pancreas occurs when there is abnormal rotation of the ventral pancreas or the duodenum, both of which must rotate for proper pancreatic positioning. Some believe that the ventral bud adheres to the duodenum, so that as the structures rotate, the ventral pancreas develops and grows around the duodenum rather than in its normal position (see figures). The ventral duct continues to drain into the major papilla and joins with the biliary system, which is its normal embryologic anatomy.
The major pancreatic complication of annular pancreas is the development of acute or chronic pancreatitis. This condition may affect as many as one quarter of patients with annular pancreas. Also, the annular pancreas produces duodenal narrowing or obstruction to varying degrees. About half of the cases of annular pancreas manifest in the neonatal period with duodenal symptoms. There may be other associated anomalies in the neonate as well. If the condition persists until adulthood, the annular pancreas may be discovered incidentally or when symptoms of pancreatitis or duodenal obstruction occur. These patients may become jaundiced as well. Surgery is necessary to correct the condition.






