History: A young man is involved in a motor vehicle accident.
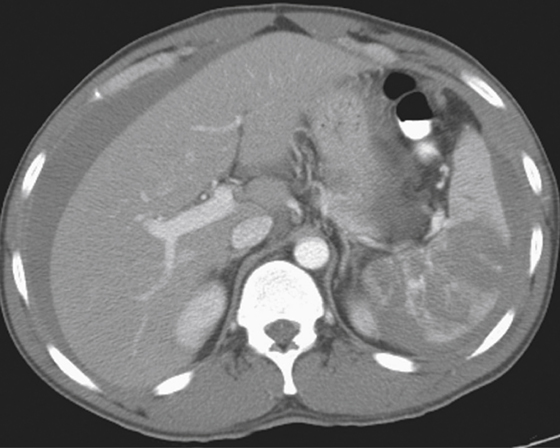
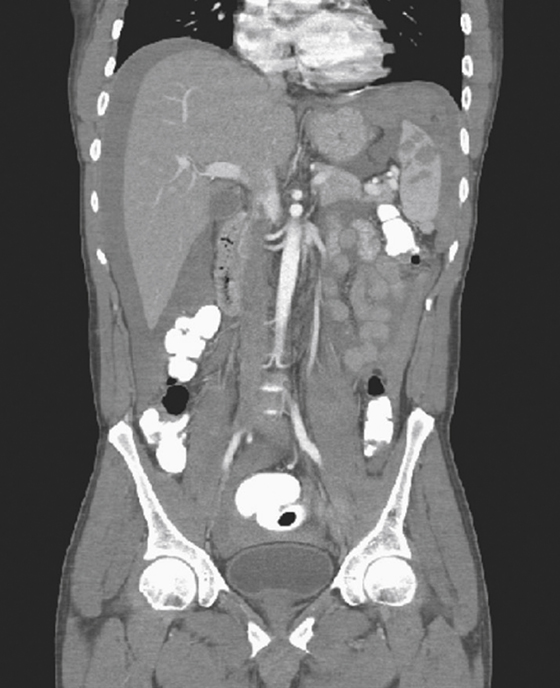
1. What is the grade of splenic injury shown on this CT scan?
2. In a patient who had trauma with splenic injury, what findings will increase the urgency of surgical intervention?
B. Multiple left rib fractures
C. Demonstration of continued bleeding
D. Presence of subcapsular hematoma
3. Which of the following complications has been reported to be associated with splenic injury and splenectomy?
B. Encapsulated bacterial sepsis
4. Which of the following is most often associated with splenic injury in blunt trauma?
ANSWERS
CASE 12
Splenic Laceration
1. C
2. C
3. B
4. B
Reference
Dahnert W. Radiology Review Manual. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2007. p 807-809
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 211.
Comment
The spleen is the most commonly injured organ in the abdomen as a result of blunt abdominal trauma, with an incidence of 25%. Historically, the treatment of choice for splenic injury was surgical, commonly splenectomy. However, splenectomy is associated with a life-long risk for potentially fatal sepsis due to encapsulated bacteria. This has led to an evolution in the management of splenic injuries to appropriately triage patients toward operative versus nonoperative management. Currently, nonoperative management of isolated blunt splenic injury is considered the standard of care for hemodynamically stable children. Patients who are hemodynamically unstable should proceed directly to surgical exploration.
Patients who are hemodynamically stable routinely receive a CT examination (see figures). The degree of splenic injury is assessed and assigned a grade. The grade will help in determining whether the patient will or will not require intervention and the need for continued evaluation of the spleen. The grading method depends on size, depth, and number of the lacerations and hematomas; amount of extravasation; and whether there is continued bleeding (see figures).
Splenic trauma is commonly graded using the Organ Injury Scaling system (American Association for the Surgery of Trauma). A grade I injury is the least-severe injury and is a subcapsular hematoma less than 10% of splenic surface area and/or a small capsular tear no deeper than 1 cm, nonexpanding, not actively bleeding. A grade V injury is a shattered spleen with involvement of the splenic vascular pedicle.






