Case 12
Teaching Points: Left Mastectomy
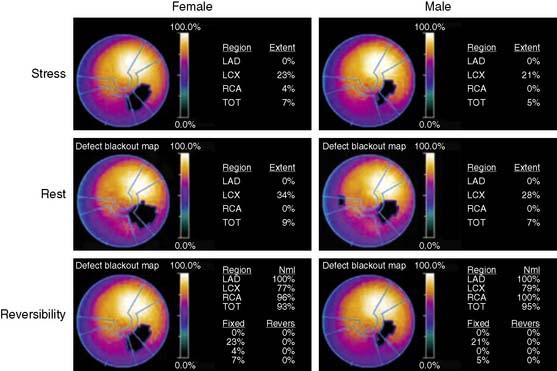
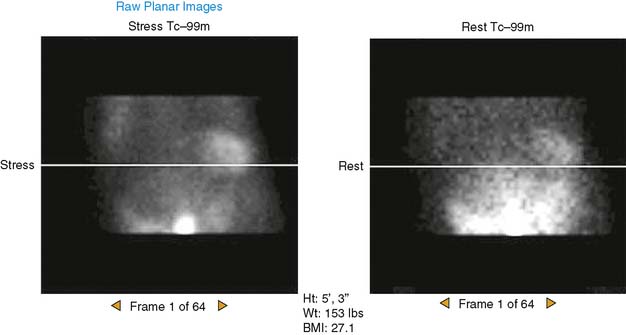
1 In women with left mastectomy, absence of the anterior attenuation produced by the left breast results in a male perfusion pattern (unopposed “diaphragmatic attenuation”).
Published on 02/03/2015 by admin
Filed under Internal Medicine
Last modified 22/04/2025
Print this pageCase 12