CASE 118
History: No patient history is available.
1. What should be included in the differential diagnosis of high signal within the outer aspect of the left ventricular cavity on black blood MRI? (Choose all that apply.)
A. Myocarditis
B. Left ventricular noncompaction
C. Sarcoidosis
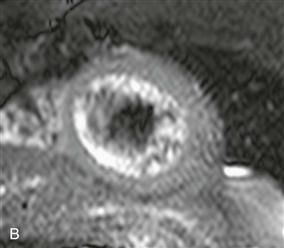
2. What is responsible for the hyperintense signal at the periphery of the left ventricular cavity on the short-axis black blood image (Fig. B)?
3. Which of the following is the most likely clinical presentation for this patient?
A. A 16-year-old boy presents with chest pain and fever following an upper respiratory tract infection.
C. A 40-year-old man presents with cardiac arrhythmia and history of a cardiac thromboembolic event.
4. What is the MRI criterion for diagnosing this condition?
A. An elevated noncompacted/compacted myocardial layer (NC/C) ratio measured at end-systole
B. An elevated NC/C ratio measured at end-diastole
ANSWERS
Reference
Yun H, Zeng MS, Jin H, et al. Isolated noncompaction of ventricular myocardium: a magnetic resonance imaging study of 11 patients. Korean J Radiol. 2011;12(6):686–692.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, p 54.
Comment
Pathophysiology
Ventricular noncompaction is a more recently described primary cardiomyopathy thought to be secondary to an arrest in myocardial development and compaction. Patients may be asymptomatic or can present with tachyarrhythmia, congestive heart failure, or cardiac thromboembolism. Ventricular noncompaction may be seen with other cardiac abnormalities including atrial septal defect, ventricular septal defect, partial anomalous pulmonary venous return, pulmonic stenosis, and Ebstein anomaly.
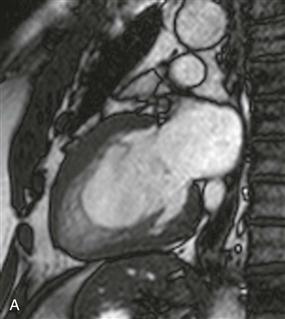
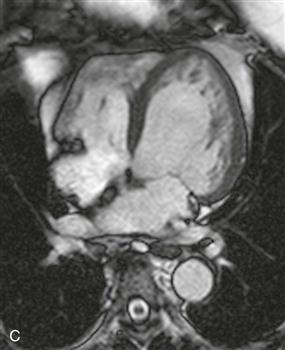
Imaging Findings, Diagnostic Criteria, and Therapy
Ventricular noncompaction most commonly affects the left ventricle. Cardiac MRI and CT findings include prominent trabeculations, deep intertrabecular recesses that communicate with the ventricular cavity, and an elevated NC/C ratio (Figs. A–C). There may be adjacent wall motion abnormality and transmural or subendocardial late gadolinium enhancement. The MRI criterion for diagnosing pathologic left ventricular noncompaction is an elevated NC/C ratio greater than 2.3 measured in end-diastole. Treatment involves aspirin in all patients to reduce the risk of systemic embolism and beta blockers and angiotensin-converting enzyme (ACE) inhibitors in patients with heart dysfunction.






