CASE 116
History: A patient presents with malaise.
1. What imaging study can be performed to evaluate the abnormality seen on the radiograph? (Choose all that apply.)
B. CT
C. MRI
D. Stress perfusion scintigraphy
2. What is the most likely diagnosis?
3. What is the most common cause of pulmonary stenosis?
A. Trauma
B. Congenital
4. What is the most common intervention for treatment of this lesion?
ANSWERS
References
Kenny D, Hijazi ZM. State-of-the-art percutaneous pulmonary valve therapy. Expert Rev Cardiovasc Ther. 2012;10(5):589–597.
Kilner PJ. Imaging congenital heart disease in adults. Br J Radiol. 2011;84(Spec No):S258–S268.
Walker CM, Reddy GP, Steiner RM. Radiology of the heart. In: Rosendorff C, ed. Essential Cardiology. ed 3 Philadelphia: Saunders; 2012.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 195–202.
Comment
Etiology and Clinical Considerations
Pulmonary valve stenosis is most commonly congenital, resulting from a valvular membrane with a central hole, a bicuspid valve, or valve dysplasia (associated with Noonan syndrome). Acquired causes include carcinoid and rheumatic heart disease.
Treatment
Balloon valvuloplasty is the most common intervention used to treat this lesion. Infants and young children are often treated with balloon valvuloplasty. One complication of balloon valvuloplasty is pulmonary regurgitation. Older children and adults usually require valve replacement.
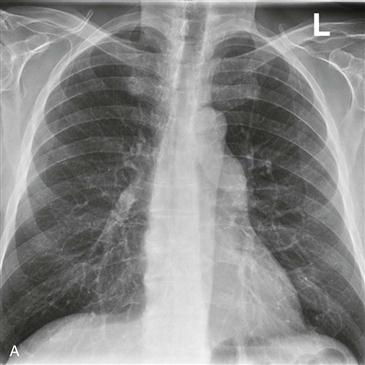
Radiography
Chest radiographic findings vary depending on patient age and associated abnormalities. In infants, a large thymus may obscure the central pulmonary arteries, and the only sign of disease may be decreased pulmonary flow. In older children and adults, there is poststenotic dilation of the main pulmonary artery (Fig. A) and often of the left pulmonary artery. The right pulmonary artery is normal. Cardiac size is usually normal, unless the stenosis is severe enough to obstruct cardiac output.
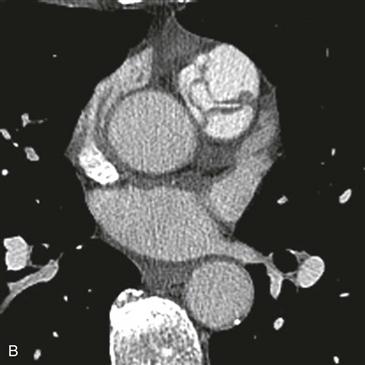
Further Imaging
Echocardiography demonstrates thickening and poor excursion of the valve leaflets and a jet across the lesion. CT and MRI can also show leaflet thickening (Fig. B) and limitation of excursion. Angiography demonstrates doming, thickening, and poor excursion of the valve leaflets. A jet of contrast agent can be seen passing across the valve.






