CHAPTER 115
Thoracic Outlet Syndrome
Definition
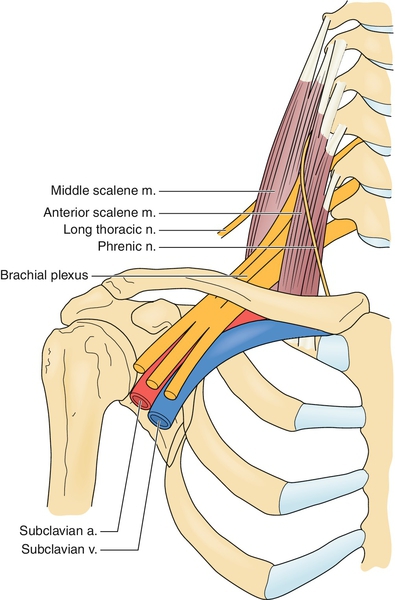
Thoracic outlet syndrome is a symptom complex caused by compression or irritation of the neurovascular structures as they leave the thoracic cage through its narrow outlet. The thoracic outlet contains many structures in a confined space. The base of the thoracic outlet is formed by the first rib and the fascia of Sibson, which is attached to the transverse process of the seventh cervical vertebra, the pleura, and the first rib. The outlet is bounded superiorly by the subclavius muscle and the clavicle, anteriorly by the anterior scalene muscle, and posteriorly by the middle scalene muscle. The brachial plexus and the subclavian artery pass over the first rib between the anterior and middle scalene muscles (Fig. 115.1).
Neurovascular compression occurs most frequently at three levels:
• in the costoscalene hiatus, bordered anteriorly by the anterior scalene muscle, posteriorly by the middle scalene muscle, and caudally by the first rib; and
• in the costoclavicular passage, bordered laterally by the clavicle, posteriorly by the scapula, and medially by the first rib.
The clinical symptoms of thoracic outlet syndrome are divided into categories according to the structures under pressure. True neurologic thoracic outlet syndrome is often caused by the distal C8-T1 roots or proximal fibers of the lower trunk of the plexus being stretched over a taut congenital band extending from the tip of a rudimentary cervical rib to the first rib. The most common form of thoracic outlet syndrome is the disputed neurologic thoracic outlet syndrome. The term disputed has been chosen because so many of the basic tenets of this syndrome are in dispute. Symptoms caused by pure venous compression (venous thoracic outlet syndrome) occur in 1.5% of patients and are manifested as axillary-subclavian vein thrombosis, usually in young patients engaged in vigorous physical activity that emphasizes upper limb and shoulder motion (such as cricket, tennis, and baseball). Arterial thoracic outlet syndrome is very rare and may be suspected if the patient presents with claudication of the arm, coldness, and ischemia of a finger or a hand. Individuals who have congenital bone or fibromuscular variations at these spaces and experience trauma are at risk for development of thoracic outlet syndrome. Anatomic variations and anomalies probably play a secondary role in the etiology. Congenital bands and ligaments are observed in a large majority of patients with thoracic outlet syndrome, and nine different types have been recognized [1]. In a human cadaver study, only 10% had a bilaterally normal anatomy. Anatomic anomalies of the thoracic-cervical-axillary region were found in 60% of human fetuses [2]. It is suggested that anatomic abnormalities confer a predisposition to symptoms of thoracic outlet syndrome after stress or injury [3]. Variation in the course of the brachial plexus that may predispose to symptoms of thoracic outlet syndrome has also been presented. Cervical ribs are regarded as predisposing factors, and a prevalence of cervical ribs was found to be 2.21% in a London population [4]. However, cervical ribs are present since birth. In 80% of patients with cervical ribs, symptoms did not develop until after a neck injury. Post-traumatic thoracic outlet syndrome has been presented in several articles [5–7].
According to Roos [1], anomalies are always the reason behind symptoms of thoracic outlet syndrome. However, only a few other surgeons have observed such anomalies. In the case of the first rib, the costovertebral and costotransverse joints allow a fair amount of rotation to take place along the long axis of the rib. Moreover, this rib has attached to it the anterior and middle scalene muscles, which act either by raising the thorax or by flexing and rotating the cervical part of the spine. In consequence, this first rib bears more stresses and strains than any of the other ribs, and these are greatest at the costotransverse joint [8]. Osteoarthritic changes are found more frequently in the costotransverse joint of the first rib. The lack of a superior supporting ligament may explain why this joint of the first rib is relatively weaker than those of the other ribs [8].
The elevation of the ribs during inspiration increases the anteroposterior diameter of the upper thorax. The range of this motion is reduced in older people. A disturbance of the function of the upper thoracic aperture will predispose to thoracic outlet syndrome symptoms. A dysfunction of the first rib at the costotransverse joint causes a restricted movement of the first rib [9]. In patients with thoracic outlet syndrome, the C8 and T1 nerve roots are most commonly affected. These roots constitute the part of the brachial plexus closest to the costotransverse joint. The stellate ganglion is located in the immediate vicinity of the first costotransverse joint and has numerous connections to the C8 and T1 roots. Minimal trauma associated with static, repetitive work, especially in young women, can cause abnormal stress on the upper aperture, and the poorly stabilized first rib can subluxate at the costotransverse joint. A subluxation at the first costotransverse joint could irritate the nerve roots C8 and T1 emerging in front of this joint. This irritation could explain the predominantly subjective pain and sensory loss in the ulnar distribution. The weakness of the hand and the various symptoms resembling complex regional pain syndrome may be explained by the irritation of the stellate ganglion.
Symptoms
True neurologic thoracic outlet syndrome is manifested with a long history of sensory symptoms, mainly along the medial forearm, associated with hand weakness and wasting, particularly of the thenar muscles (Fig. 115.2). In the upper plexus type presented by Roos [1], pain is felt over the brachial plexus radiating from the ear, through the anterior cervical region, over the clavicle into the upper part of the chest, posteriorly into the rhomboid and scapular areas, across the trapezius, and down the outer arm into the radial aspect of the forearm in a C5-C6 distribution. In the lower plexus type, pain is felt in the supraclavicular and infraclavicular fossae, radiating into the upper part of the back and from the axilla down the inner arm along the ulnar nerve distribution.

In contrast, disputed neurologic thoracic outlet syndrome possesses none of these characteristics. The most common symptoms are pain and paresthesias in an ulnar distribution and numbness, tingling, weakness, or dysfunction of the hand. The list of symptoms attributed to disputed neurologic thoracic outlet syndrome is long. These patients are often told by their physicians that their symptoms are exaggerated or that their complaints are not real. Coldness, easy fatigability, ischemia of a finger or a hand, and pallor on elevation are considered to be symptoms of arterial origin. Swelling, discoloration, and a heavy feeling in the hand are considered to be symptoms of venous origin. Swelling, hyperesthesia, discoloration, and a feeling of alternate cold and warm could also be signs of complex regional pain syndrome. Traction on the stellate ganglion has also been considered a possible cause of pain in these patients [8]. In general, in the absence of peripheral emboli, most “vascular symptoms” or “Raynaud phenomena” probably result from irritation of the sympathetic nerves rather than from compression of the subclavian artery in the thoracic outlet. A common feature of the symptoms is their intermittence and provocation by use of the arm above shoulder level. Aggravation of the symptoms often occurs after rather than during exercise.
Physical Examination
The diagnosis of thoracic outlet syndrome is a clinical one based on a detailed history and physical examination. This takes time and effort. Years of inappropriate diagnosis and ineffective therapy take a heavy toll on these patients. In the physical examination, the individual as a whole must be taken into consideration. One must remember that many of these patients have some psychological complaints. A thorough clinical examination including a logical explanation for the symptoms will often relieve the psychic burden.
The physical examination starts with an inspection of the neck, shoulders, and upper extremities. Color, muscle atrophy, edema, temperature, and nails are examined. This examination requires the patient to be examined with the shirt off. The cervical spine is then examined to exclude symptoms of cervical origin caused by a cervical disc or spondylarthrotic intervertebral foramen. A typical pain radiculation in C5 to C8 distribution indicates that a nerve root irritation is present. A local distribution of pain with neck extension indicates a facet joint problem.
A neurologic examination is performed to include sensory testing, muscle strength testing (C5-C8), and reflexes. Tinel sign is tested to exclude carpal tunnel syndrome. Palpation of the median, ulnar, and radial nerves from the axilla to the hand may reveal tenderness. This tenderness will vanish if a successful therapy is administered [10].
Almost all clinical tests used in the examination of the patient with thoracic outlet syndrome aim to provoke the symptoms felt by the patient, presuming that the compressing structure may be provoked to irritate the neurovascular bundle in the area of the thoracic outlet during the test. These maneuvers are unreliable in general [11]. A clinical test in extensive use is the Adson test [12]. With the patient sitting, hands resting on the thighs, both radial pulses are simultaneously palpated. During forced inspiration, hyperextension of the neck, and turning of the head to the affected side, the radial pulse is palpated for obliteration, and auscultation is done for supraclavicular bruit. The test has changed during the years. In 1927, when Adson described his test, the vascular changes were considered to be pathognomonic of thoracic outlet syndrome. Later, neurologic changes occurred more frequently than vascular ones, and these can be detected better when the head is rotated to the contralateral rather than the ipsilateral side, as initially described.
Radial pulse obliteration or subclavian bruit is found in 69% of normal patients [13]. All studies clearly indicate that pulse obliteration with the arm and head in various positions is a normal finding and has no relation to thoracic outlet syndrome.
In the hyperabduction test, symptoms are reproduced by hyperabduction of the arm. However, more than 80% of normal individuals experience obliteration of the radial pulse during this test [14]. In the exaggerated military maneuver, also called Eden test, symptoms are reproduced by pulling back the acromioclavicular joint in an exaggerated military “attention” position. The neurovascular structures could be compressed between the first rib and the clavicle, without any anatomic predisposing factors. This maneuver is also referred to as the costoclavicular test. Arterial compression is found in 60% of asymptomatic individuals by this test.
In the abduction–external rotation test, also called Roos test or elevated arm stress test (EAST), the hands are in the “stick up” position and are then repeatedly opened and closed for 3 minutes. Roos [1] considered the symptoms to be due to both arterial and brachial plexus compression and referred to this procedure as a claudication test; he was later convinced that thoracic outlet syndrome was neurologic rather than vascular in origin but claimed that the EAST procedure was the most reliable procedure. Roos has also claimed that the EAST procedure has great specificity, with a positive result in thoracic outlet syndrome but generally negative results in carpal tunnel syndrome and cervical radiculopathy. However, in a controlled study, it was found that the EAST procedure is an excellent test for carpal tunnel syndrome; the result is positive in 92% of patients with carpal tunnel syndrome and in 74% of normal controls [15]. Positional compression during all of these tests is a common phenomenon in normal subjects, and diminishing of the pulse in Adson test, the costoclavicular maneuver, and the hyperabduction test is considered to be a normal finding rather than a pathologic one. None of these tests unequivocally establishes the presence or absence of thoracic outlet syndrome. Ribbe and colleagues [16] used a “thoracic outlet syndrome index” to establish the diagnosis of thoracic outlet syndrome. According to these authors, a patient with thoracic outlet syndrome should have at least three of the following four symptoms or signs:
1. A history of aggravation of symptoms with the arm in the elevated position
2. A history of paresthesia in the segments C8-T1
3. Tenderness over the brachial plexus supraclavicularly
4. A positive “hands-up” (abduction–external rotation) test result
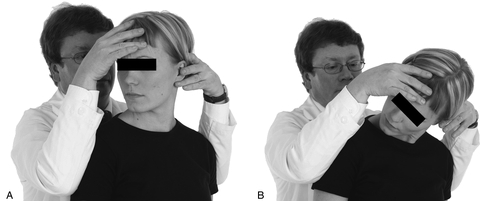
Because all of these provocative maneuvers are unreliable, one should examine the function of the thoracic upper aperture. The function of the upper thoracic aperture should be analyzed with the cervical rotation–lateral flexion test [17]. The test is carried out as follows. The neutrally positioned cervical spine is first passively and maximally rotated away from the side being examined and then, in this position, gently flexed as far as possible, moving the ear toward the chest. This is done in both directions. A restriction blocking the lateral flexion part of the movement indicates a positive test result; a free movement indicates a negative test result (Fig. 115.3). This test indicates an abnormal function of the upper thoracic aperture. The test is indicative of a subluxation of the first rib at the costotransverse joint. The test has been used to identify patients who did not gain from surgery [18] as well as in a 2-year follow-up study after conservative treatment [10].
In the surgery series [18], it was hypothesized that the remaining stump of the first rib was subluxated and that is why the symptoms persisted after surgery. The importance of the length of the remaining stump has also been stressed by other authors [19,20]. It is mandatory to analyze the function of the upper thoracic aperture and not rely only on provocative maneuvers that may lead to unnecessary surgical interventions.
Functional Limitations
The patients with symptoms of thoracic outlet syndrome have difficulty in working over the horizontal level, such as cleaning windows and putting up draperies. Static work, such as working with a keyboard, may be difficult because of paresthesias and difficulty in controlling the movements of the arm. Many patients cannot “rely” on the hand. Sleep is disturbed because of pain and tingling after exertion during the day.
Diagnostic Studies
Radiologic examination in the thoracic outlet syndrome can detect cervical ribs, bone anomalies of the first or second ribs, tumors, or the “droopy shoulder” syndrome. The incidence of arterial compression of clinical significance is extremely low, and arteriography should not be used in the diagnosis of thoracic outlet syndrome, except in patients with signs of pronounced compression or ischemia. Arterial compression inside the thoracic outlet can be detected with Doppler ultrasonography.
Magnetic resonance imaging has been used to detect anomalies, but these may not correlate with symptoms [21]. Functional magnetic resonance imaging may show a smaller distance between the first rib and the clavicle, but the significance remains to be shown. A cineradiographic study can detect abnormal movement of the structures of the upper aperture, but this can be detected with clinical tests [17].
Somatosensory evoked potentials can document the neurocompressive component of thoracic outlet syndrome and provide an objective assessment. The theory of the “double crush” syndrome suggests that nerve compression at one level makes the whole nerve more vulnerable to compression injury at another level. Symptoms after an unsuccessful carpal tunnel operation disappeared after a first rib excision [22]. The double crush phenomenon should be taken into account and neurophysiologic examination should be performed to exclude more distal sites of nerve compression than the thoracic outlet, such as nerve entrapment in the carpal tunnel.
Treatment
Initial
After the thorough clinical examination and detailed history (including the question, “Have you had a trauma to your neck region?”) [5,6,23], what the examining physician suspects to be the origin of the symptoms must be explained to the patient. Good pain management, not only using pain medications but also taking into account sleeping hygiene, is important. A multiprofessional team [24] should be consulted so that all therapy modalities are taken into account. This includes physiatrists, physiotherapists, occupational therapists, social workers, and psychologists; also, there must be a possibility to consult specialists in neurology and psychiatry, thoracic surgeons, and neurosurgeons.
Rehabilitation
The outcome of conservative therapy varies among different studies. Sällström and Celegin’s program [25] brought relief to 83% of patients with mild symptoms but only 9% of those with severe symptoms. Even a success rate of 100% has been reported (a supervised physiotherapy program of graduated resisted shoulder elevation exercises in eight patients). Almost all authors have emphasized exercises to improve patients’ posture as well as strengthening exercises of the shoulder girdle. However, it is difficult to compare the different studies because the diagnostic criteria are seldom mentioned, the severity of the symptoms varies, and rarely is the type of therapy described.
Procedures
During the last 25 years, I have recommended and used a multidisciplinary approach [10]. The therapy itself starts with shoulder exercises, the purpose of which is to restore the movement of the whole shoulder girdle and to provide more space for the neurovascular structures. Restoration of the movement and function of the cervical spine follows. The exercises that aim to activate the anterior, middle, and posterior scalene muscles are the most important part (Fig. 115.4). These exercises have been shown to correct any malfunction of the first ribs, thus normalizing the function of the upper thoracic aperture [26] and enabling normal movement of the first ribs. Stretching of the muscles of the shoulder girdle involves the upper part of the trapezius muscles, the sternocleidomastoid muscles, the levator scapulae, and the small pectoral muscle. The role of the small pectoral muscle has been emphasized elsewhere [27]. Further stretching exercises should be administered as needed, depending on the clinical findings in the individual case. Strengthening exercises for the anterior serratus muscle should be included, thus enhancing the stability of the scapula. Nerve gliding exercises are used to restore the mobility of the nerves. It is mandatory that physiotherapists, psychologists, occupational therapists, and social workers be consulted during the whole process. The patients should be observed for a long time because relapses are common. With use of this program, I found that 88.1% of the patients were satisfied with the outcome, that is, their symptoms had either disappeared or were much abated or the real cause of the symptoms had been diagnosed.

Recommendations were carried through during a 2-year follow-up period in 87.9% of cases. Of the patients who were advised to retire because of symptoms, the primary problem was found to be other than thoracic outlet syndrome (psychiatric causes, complex regional pain syndrome, polyneuropathy, multiple sclerosis, other) [10]. Conservative therapy is the treatment of choice in thoracic outlet syndrome because it is safe and can be implemented as a self-treatment program.
If symptoms are not abated despite restored function, the differential diagnosis should be reviewed. The fact that conservative treatment is tedious and relapses are common should not be considered a reason for surgical intervention. Surgery is a viable option only if there are signs of significant motor loss, atrophy, or vascular thrombosis. Psychosocial aspects should always be taken into account. It is extremely important to evaluate the degree of disability that thoracic outlet syndrome symptoms cause in relation to the patient’s life situation and psychosocial abilities.
There is a link between the workplace and the individual in the pathogenesis and course of thoracic outlet syndrome. The role of occupational factors must be considered, and one has to go back to “the scene of the crime.”
Surgery
Cherington [28] stated already in 1991, “It is important for surgeons and primary care physicians to be aware of the rising tide of skepticism surrounding the diagnosis and treatment of the thoracic outlet syndrome.” Skepticism is indeed justified for several reasons. The most often diagnosed and surgically treated form of thoracic outlet syndrome in the United States, disputed neurologic thoracic outlet syndrome, has no objective clinical, radiologic, or electrodiagnostic criteria. In 1927, Adson [12] introduced scalenotomy as an approach to relieve structures from compression. Roos [1] presented a transaxillary resection of the first rib, and this operation has perhaps been the most used approach. Supraclavicular approaches have also been presented. Some authors claim the results of surgical management to be good, excellent, or favorable in more than 90% of patients [29]. Different studies, however, are difficult to compare because of the various criteria used to assess the outcome. In addition, the numbers of patients have ranged from 26 to 1336 and the follow-up times from 1 month to 15 years. Some authors do not state the follow-up time at all. A combined surgical treatment using transaxillary first rib resection and transcervical scalenotomy is said to be more effective than either of these alone [30]. There have been only a couple of studies in which the follow-up examination was done by independent examiners not involved in the surgical procedure or selection of the patients. This seems to affect the results after surgery. Among the different operative procedures, scalenotomy seems to speed up patients’ retirement [31]. Cuetter and Bartoszek [32] and Lindgren [18] have reevaluated patients treated unsuccessfully with surgery for thoracic outlet syndrome; they found that in each case, another disease or functional disturbance explained the patient’s complaints.
Recurrence after unsuccessful procedures may be a disabling and difficult problem for patients. This is extremely tragic in patients who have been found to have pulse changes in provocative positions in the absence of any other symptoms. Even abnormal electrodiagnostic findings before an operation do not predict the outcome of surgery [33]. Clinical tests show a good sensitivity but a poor specificity and cannot be used as the predictors for the outcome after surgery [34]. Long-term results of operation for thoracic outlet syndrome may be much worse than those initially achieved. Patients who present with poorly systematized neurologic symptoms have poor results after surgery and should be denied surgery or at least informed that postoperative results may be disappointing [35].
Botulinum chemodenervation of the scalene muscles has been found useful in alleviating symptoms in patients with thoracic outlet syndrome, especially if they are waiting for definitive surgical decompression. However, a randomized trial showed that chemodenervation did not result in clinically or statistically significant improvement in pain, paresthesias, or function in a population with thoracic outlet syndrome [36].
Potential Disease Complications
It is very important to detect those patients with post-traumatic thoracic outlet syndrome. These may present with worsening of the symptoms, such as a decrease in muscle strength, increase of pain, and tingling in the radicular territory, as well as unspecific disturbances, such as dizziness and face pain. In the case of these patients, one must consider surgical options [23]. It has been said that true neurogenic thoracic outlet syndrome is rare. Overdiagnosis of this syndrome results from a failure to realize that a wide range of symptoms occur regularly in patients with carpal tunnel syndrome and that these are commonly outside the anatomic distribution of the median nerve. The failure to recognize this can reinforce abnormal behavior in patients, particularly when they are subjected to unnecessary brachial plexus or ulnar nerve surgery, undertaken without neurophysiologic identification of an appropriate neurogenic abnormality [37]. If they are not dealt with correctly, these patients will suffer for long periods with more than one symptom. These may include muscle atrophy, swelling in the supraclavicular fossa, abnormal posture, and tendency to faint with certain movements. The leading symptom is numbness and clumsiness of the hand, but pain in the occiput-shoulder area is an important symptom too [38]. These may worsen without proper therapy.
Potential Treatment Complications
Surgery for thoracic outlet syndrome is not as innocuous as it was once thought. Dale [39] found that more than half of those who reported performing the surgery had encountered brachial plexus injuries severe enough to produce clinical weakness, nearly one fifth of which were permanent. Large numbers of failed thoracic outlet syndrome surgery have been reported during the last decades. Brachial plexus lesions, infections, and cases of life-threatening hemorrhage have been published. Even deaths have been reported. Franklin and colleagues [40] reported that 60% of workers were still work disabled 1 year after thoracic outlet syndrome decompression surgery.






