[level-membership-for-gastroenterology-and-hepatology-category]CASE 115

History: A 58-year-old man presents with nausea and dyspepsia.
1. What should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
2. Which of the following statements regarding Ménétrier’s disease is true?
A. The etiology of Ménétrier’s disease is unknown.
B. Ménétrier’s disease progresses to malignancy if uncontrolled.
C. Ménétrier’s disease responds dramatically to steroid treatment.
D. Fold changes occur only in the proximal stomach.
3. Which of the following statements regarding eosinophilic gastritis is true?
A. About half of patients have a peripheral eosinophilia.
B. The small bowel is the most common site of involvement.
C. There is usually associated colonic disease.
D. This condition responds well to steroid treatment.
4. Which of the following statements regarding gastric sarcoidosis is true?
A. There is always associated pulmonary disease.
B. Gastric involvement is a rare complication of sarcoidosis.
C. Steroid treatment is valuable for pulmonary disease but not gastric involvement.
D. The small bowel is the most common site of involvement of the gastrointestinal (GI) tract.
ANSWERS
CASE 115
Ménétrier’s Disease of the Stomach
1. A, B, D, and E
2. A
3. D
4. A
References
Friedman J, Platnick J, Farruggia S, et al: Ménétrier’s disease. Radiographics. 2009;29(1):297–301.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 70.
Comment
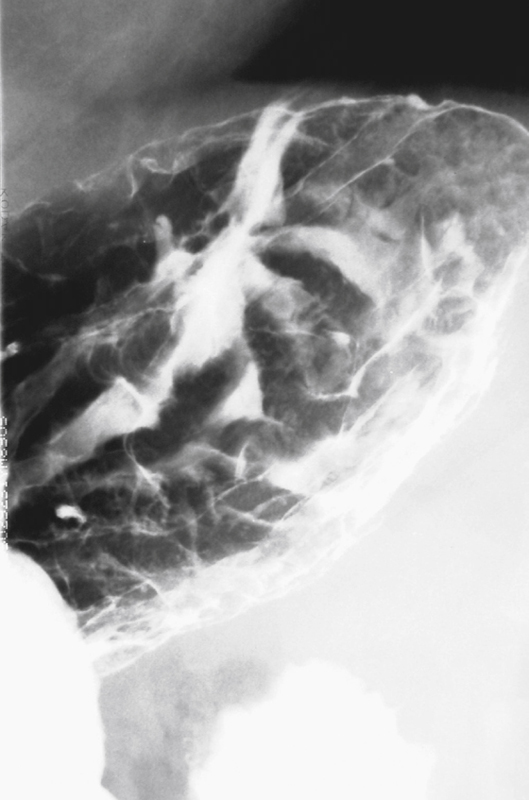
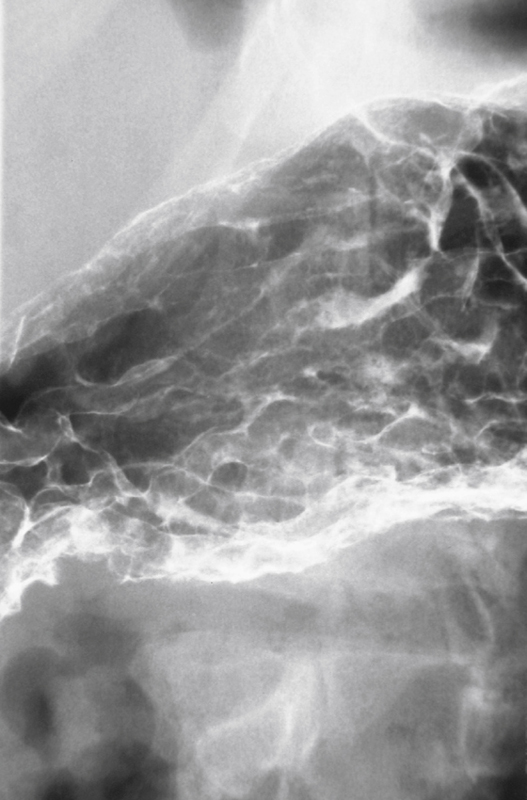
Thickened gastric folds are a common radiologic finding that can be produced by many unusual disorders. The imaging finding itself is so nonspecific that all of the various disorders cannot be distinguished by their radiologic appearance (see figures).
Ménétrier’s disease is a rare condition in which marked glandular hypertrophy of the stomach develops without any underlying cause. There is associated enlargement of the gastric rugae, hypochloremia, and hypoproteinemia. Despite the fact that there is often increased mucus secretion in the stomach, gastric acid output is reduced, which differentiates the disease from other types of hypertrophic gastritis in which acid output is often elevated. Protein-losing enteropathy is another distinguishing characteristic of Ménétrier’s disease. Patients often have pain, weight loss, vomiting, and diarrhea. According to the classic description of the disease, the hypertrophic fold changes occur only in the proximal stomach, but it is now known that the thickened folds can be seen throughout the stomach, including the antrum.
Spontaneous remission can occur, but often Ménétrier’s disease is a chronic recurrent illness that responds poorly to various therapies (e.g., antibiotics, H2 blockers). In severe cases, gastric resection may be required. There is controversy regarding whether the condition is premalignant. The prevailing thought is that it is not.
In a patient with peripheral eosinophilia and thickened gastric folds, eosinophilic gastritis should be strongly considered. There is often associated small bowel disease in patients with fold thickening. Sarcoidosis of the stomach may be more common than first appreciated; according to some reports, the condition can be identified in 10% of gastric biopsy specimens. With sarcoidosis, there is always associated pulmonary disease, and other portions of the GI tract may be involved. Both of these conditions respond dramatically to steroids, as do a few other gastric conditions.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 115
History: A 58-year-old man presents with nausea and dyspepsia.
1. What should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
2. Which of the following statements regarding Ménétrier’s disease is true?
A. The etiology of Ménétrier’s disease is unknown.
B. Ménétrier’s disease progresses to malignancy if uncontrolled.
C. Ménétrier’s disease responds dramatically to steroid treatment.
D. Fold changes occur only in the proximal stomach.
3. Which of the following statements regarding eosinophilic gastritis is true?
A. About half of patients have a peripheral eosinophilia.
B. The small bowel is the most common site of involvement.
[/not-level-membership-for-gastroenterology-and-hepatology-category]
