CASE 113
History: A 55-year-old woman presents with vomiting and weight loss.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the most common cause of gastric outlet obstruction?
3. Which of the following statements regarding gastric outlet obstruction is false?
A. Caustic ingestion frequently leads to gastric outlet obstruction.
B. Transpyloric prolapse of gastric mucosa is usually asymptomatic.
C. Patients with gastroduodenal involvement by Crohn’s disease are usually symptomatic.
D. Gastric outlet obstruction is the most common complication of gastroduodenal tuberculosis.
4. What condition results in gastric obstruction secondary to a gallstone lodged in the pyloric channel?
ANSWERS
CASE 113
Gastric Outlet Obstruction Caused by Metastatic Disease
1. A, B, C, and E
2. A
3. C
4. D
References
Dahnert W. Radiology Review Manual. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2007. pp 760-761
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 49.
Comment
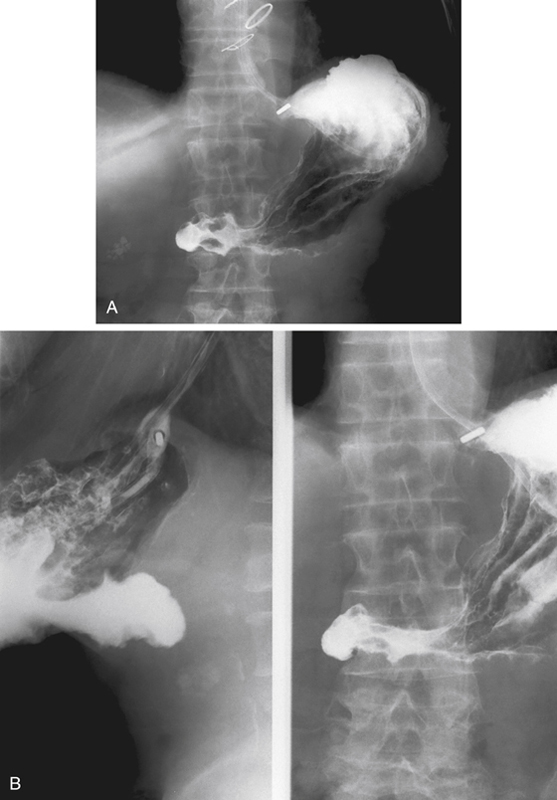
In pediatric patients, especially boys in the first year of life, pyloric hypertrophy with stenosis is a common cause of gastric outlet obstruction and is usually easily diagnosed on ultrasound. However, in older patients, pyloric hypertrophy is very rare. The most common cause of gastric outlet obstruction in adults is probably malignancy, primary and secondary. The usual lesion is pancreatic or peripancreatic. In this case, the lesion was widespread metastatic disease that had invaded the duodenum. Primary carcinoma involving the head of the pancreas is often the obstructing lesion. Pancreatic carcinoma can also invade the stomach itself, but this seldom causes outlet obstruction. Primary duodenal lesions can result in outlet obstruction.
Barium upper GI studies can establish the presence of a mechanical cause of gastric distention and may suggest the cause (see figures). Upper GI endoscopy can do the same with the added benefit of biopsy, if indicated. Multiplanar CT has become an outstanding tool in the work-up of these patients and is being used with increasing frequency. CT evaluation also includes the surrounding structures and the entire peritoneal cavity. Whatever diagnostic pathway is used, multiplanar multidetector CT is usually the eventual imaging choice. MRI is being used with more frequency but is still far behind CT in terms of time, cost, and availability.






